
Archived - Evaluation of Community-Based Healing Initiatives Supported Through the Aboriginal Healing Foundation
Archived information
This Web page has been archived on the Web. Archived information is provided for reference, research or record keeping purposes. It is not subject to the Government of Canada Web Standards and has not been altered or updated since it was archived. Please contact us to request a format other than those available.
Date: December 7, 2009
PDF Version (1.63 MB, 72 pages)
Table of Contents
- Acronyms
- Executive Summary
- Management Response / Action Plan
- 1.0 Introduction
- 2.0 Evaluation Methodology
- 3.0 Evaluation Findings
- 4.0 Cost Effectiveness
- 5.0 Future Directions
- 6.0 Conclusions
- 7.0 Recommendations
- Literature & Documents Consulted
- Appendix A
Acronyms
| AFN | Assembly of First Nations |
|---|---|
| AHF | Aboriginal Healing Foundation |
| CEP | Common Experience Payment |
| DOJ | Department of Justice |
| GOC | Government of Canada |
| FNITP | First Nations and Inuit Transfer Payments (Information System) |
| HC | Health Canada |
| IAP | Independent Assessment Process |
| INAC | Indian and Northern Affairs Canada |
| IRS | Indian Residential Schools |
| ITK | Inuit Tapiriit Kanatami |
| IRSRC | Indian Residential Schools Resolution Canada |
| MNC | Métis National Council |
| PALO | Department of Public Affairs, Liaison and Outreach |
| PSEPC | Public Safety and Emergency Preparedness Canada |
| RBAF | Results-based Audit Framework |
| RMAF | Results-based Management and Accountability Framework |
| SA | Settlement Agreement |
| SAISC | Settlement Agreement Implementation Steering Committee |
| SOW | Statement of Work |
| TOR | Terms of Reference |
| TRC | Truth and Reconciliation Commission |
Executive Summary
Introduction
The following report presents the findings of an evaluation undertaken by DPRA Canada in association with T.K Gussman Associates, on behalf of Indian and Northern Affairs Canada, of the community-based initiatives of the Aboriginal Healing Foundation (AHF) for the period April 2007 to May 2009.
The AHF, begun in 1998 in response to recommendations arising from the Royal Commission on Aboriginal Peoples and the Government's subsequent Action Plan, "Gathering Strength", has had the principal objective of healing Aboriginal individuals, families and communities of the effects of abuses and cultural losses suffered as a result of attendance at Indian Residential Schools (IRS). Over the ten year period, the Government of Canada (GOC) has contributed $515 million to the AHF to support this objective. The last contribution was in the form of an additional $125 million in funding that arose from the Indian Residential Schools Settlement Agreement (IRSSA) and covers the period from 2007-2009.
The model followed by the AHF has been to fund community-driven and culturally-based projects that use a variety of healing methods and models, in response to community needs. The evaluation is part of the terms of the IRSSA and the Funding Agreement between the AHF and the GOC, which outlines the Minister's right to conduct a program evaluation.
The primary objective of the evaluation has been to assess the effectiveness, impacts, cost-effectiveness and continued relevance of the healing initiatives and programs undertaken by the AHF under the Settlement Agreement for the period under review, and provide evidence that will support the Government's decision-making regarding whether and to what extent funding should continue beyond the current end date of March 2010 for some projects and March 2012 for others (the 11 healing centres currently funded).Methodology
The evaluation took place over a very condensed time period between June and September of 2009. The methodology pursued a number of lines of evidence, as follows:
- Review of 108 documents and literature sources;
- Review of Administrative files (Annual and quarterly reports for 07/08 and 08/09 for a sample of 29 AHF-funded projects (including the eight case study projects);
- 35 Key informant interviews of individuals from the following groups: AHF; relevant government departments; Aboriginal organizations; project directors from AHF-funded projects outside the case study sample; and subject experts from across Canada; and
- Eight Community case studies conducted on-site at locations across Canada. During the case studies, a total of 145 interviews were conducted with participants and key stakeholders.
Highlights of Evaluation Findings
Program Effectiveness:
There is almost unanimous agreement among those canvassed that the AHF has been very successful at both achieving its objectives and in governance and fiscal management.
A number of indicator measures provide evidence that AHF healing programs at the community level are effective in facilitating healing at the individual level, and are beginning to show healing at the family and community level. AHF research has shown that it takes approximately ten years of continuous healing efforts before a community is securely established in healing from IRS trauma.
Program enrolment is growing at an average of 40 percent in the projects reviewed, and case study sites report growing enrolments and increased demand for healing services. Project data show that enrolments include increasing ratios of historically hard-to-reach groups such as youth and men.
Although evidence points to increasing momentum in individual and community healing, it also shows that in relation to the existing and growing need, the healing "has just begun". For Inuit projects in particular, the healing process has been delayed due to the later start of AHF projects for Inuit.
The majority of projects note they are not sustainable without AHF funding, although efforts are being made in some cases to secure funding from other sources; however, as there are no other agencies with a matching mandate, funding partners are difficult to find.
Program Impacts:
Impacts of the programs are reported as positive by the vast majority of respondents, with individual impacts ranging from improved family relationships, increased self-esteem and pride; achievement of higher education and employment; to prevention of suicides. Reported community impacts are growth in social capital indicators such as volunteerism, informal caring networks, and cultural events. One of the notable impacts reported by case study communities is that the "silence" and shame surrounding IRS abuses are being broken, creating the climate for ongoing healing. Projects report that capacity for healing has been built in communities and between communities; an example of such inter-community capacity growth is the sharing of best practices that has occurred between communities in both formal and informal ways, supported by the AHF and undertaken by projects on their own.
Impacts of the GOC Apology and Settlement Agreement:
Although reaction to the GOC Apology was mixed, the evaluation found that the majority of respondents felt it played a major role in creating awareness of IRS issues in the general public, and for many former IRS students and their families, provided the acknowledgement and validation of their suffering they had been looking for.
The Common Experience Payment and Independent Assessment Process are increasing the need for healing by "opening up" the issue for many Survivors for the first time. AHF projects and Survivor Societies are seeing a significant increase in demand for services in relation to these processes.
Continued Relevance of AHF Healing Programs:
Project reports show that healing program reporters identify an array of negative social indicators and challenges to healing that persist in their communities. Evaluation evidence from case studies shows that almost 90 percent of respondents estimate that "more than 50 percent" of their community members need healing from the effects of IRS. The estimated high level of need, together with the growing program enrolments and the anticipation that the Settlement Agreement processes will continue for at least another three years, support the argument for the continued relevance of AHF healing programs. The evaluation results strongly support the case for continued need for these programs, due to the complex needs and longterm nature of the healing process.
Given the Settlement Agreement commitment by the GOC, and keeping in mind the assessments of the number of Survivors and intergenerationally impacted who are anticipated to need support; and the fact that Health Canada support programs are designed to provide specific services that are complementary but different to those of the AHF; and the reported numbers of Survivors seeking help from AHF and Survivor Societies, the logical course of action for the future would seem to be continuation of support for the AHF. This support is needed at least until the Settlement Agreement compensation processes and commemorative initiatives are completed, and ideally, beyond, until indicators of community healing are much more firmly established and Aboriginal people and communities either no longer need such supports, or are able to achieve healing from IRS effects through other means. Expert key interviewees note that there is presently no equivalent alternative that could achieve the desired outcomes with the rate of success the AHF has achieved.
Recommendations
It is recommended that:
1. The Government of Canada should consider continued support for the Aboriginal Healing Foundation, at least until the Settlement Agreement compensation processes and commemorative initiatives are completed.
2. The Government of Canada explore options with the Aboriginal Healing Foundation to determine how best to maximize any additional resources, should they become available, in order to be better able to meet the healing needs of Aboriginal Canadians.
3. The Government of Canada undertake a study, in partnership with the Aboriginal Healing Foundation, research organizations, and stakeholders, to determine the healing needs of Aboriginal Canadians post Indian Residential Schools Settlement Agreement and determine whether funding should be continued and, if so, to what extent, and what role, if any, the Government of Canada should play.
4. The Government of Canada implements, in the funding agreement with the Aboriginal Healing Foundation, a requirement to collect data to help determine cost effectiveness of community-based healing projects supported by the Foundation. They should also examine the possibility of a mandate to conduct strategic research and evaluation activities; however, this enhanced mandate should not detract from funding that would normally flow to community-based projects.
Management Response & Action Plan
Project Title: Evaluation of Community-Based Healing Initiatives Supported through the Aboriginal Healing Foundation
Project Number: 1570-7/08042
Region or Sector: Resolution and Individual Affairs
| Recommendations | Actions | Responsible Manager | Planned Implementation and Completion Dates |
|---|---|---|---|
| 1. The Government of Canada should consider continued support for the Aboriginal Healing Foundation, at least until the Settlement Agreement compensation processes and commemorative initiatives are completed. | INAC will explore the feasibility of developing a policy proposal to support the Aboriginal Healing Foundation, taking into account the needs of survivors, their families and their communities. | Director General, Policy, Partnerships and Communications Branch | March 31, 2010 |
| 2. The Government of Canada explore options with the Aboriginal Healing Foundation to determine how best to maximize any additional resources, should they become available, in order to be better able to meet the healing needs of Aboriginal Canadians. | INAC will explore, in consultation with Health Canada and the Aboriginal Healing Foundation, how best to maximize the benefits/healing needs of Aboriginal Canadians should additional resources become available. | Director General, Policy, Partnerships and Communications Branch | March 31, 2010 |
| 3. The Government of Canada undertake a study, in partnership with the Aboriginal Healing Foundation, research organizations, and stakeholders, to determine the healing needs of Aboriginal Canadians post Indian Residential Schools Settlement Agreement and determine whether funding should be continued and, if so, to what extent, and what role, if any, the Government of Canada should play; and | INAC commits to undertake a study, in partnership with the Aboriginal Healing Foundation, research organizations and stakeholders, to assess the healing needs of Aboriginal Canadians. INAC will raise this issue with existing fora to determine what role Canada could play in the healing needs of Aboriginal Canadians. | Director General, Policy, Partnerships and Communications Branch | March 31, 2012 |
| 4. The Government of Canada implement, in the funding agreement with the Aboriginal Healing Foundation, a requirement to collect data to help determine cost effectiveness of community-based healing projects supported by the Foundation. They should also examine the possibility of a mandate to conduct strategic research and evaluation activities; however, this enhanced mandate should not detract from funding that would normally flow to community-based projects. | INAC will include a requirement to collect data to help determine cost effectiveness of community-based healing projects supported by the AHF. Should resources become available, INAC will explore the possibility of expanding the mandate of the Aboriginal healing Foundation to develop and implement a strategic research and evaluation plan. |
Director General, Policy, Partnerships and Communications Branch | March 31, 2010 |
1.0 Introduction
Indian Residential Schools (IRS) officially operated in Canada from 1892 to 1996, either entirely government-administered, or through funding arrangements between the Government of Canada (GOC) and the major Christian churches of the period. Thousands of Aboriginal people who attended these schools have reported that physical, emotional, and sexual abuses were widespread in the school system. [Note 1] The equally powerful cause of trauma reported by former students, their families, and their descendants is the loss of culture and language, and the lifelong effects on people who, as children, were institutionalized in settings alien to them, away from their families and social networks.
The legacy of this trauma has reverberated through Aboriginal communities until the present. By one estimate, there are approximately 86,000 of these Survivors still living in Canada. [Note 2] The Royal Commission on Aboriginal Peoples recommended that Canada take action to address these impacts on individuals, families and communities, and the GOC's "Gathering Strength – Canada's Aboriginal Action Plan" [Note 3], recommends "a healing strategy to address the healing needs of Aboriginal People affected by the Legacy of IRS, including the intergenerational impacts" [Note 4]
1.1 Program Description
The federal government provided a $350 million grant in 1998 for community-based healing of residential school trauma, and on March 31, 1998, the Aboriginal Healing Foundation (AHF) was created, with a ten year mandate. Before the end of the initial ten year funding period, the federal government subsequently provided an additional $40 million for 2005-2007. Since 1998, the GOC has contributed $515 million to the AHF to support the objective of addressing the healing needs of Aboriginal People affected by Residential Schools.
As part of the Indian Residential Schools Settlement Agreement (IRSSA) reached through a judicial process involving a number of parties, the GOC provided an additional $125 million endowment, [Note 5], to apply to the AHF for the period from April 1, 2007, to March 31, 2012. The AHF applied this $125 million to existing AHF projects. The $125 million has extended funding for existing projects for three years (ending March 31, 2010) and for eleven healing centers for four and a half years (ending March 31, 2012). The funding allocation and the time frame between April 1, 2007, and May 2009 are the focus of this evaluation.
The Foundation, which is an Aboriginal-operated, not-for-profit corporation, operates independently of government, and has administered the fund in accordance with a Funding Agreement between the Foundation and the GOC. The intention from the outset has been that the AHF not duplicate existing services provided "by or within funding from federal, provincial or territorial governments." [Note 6]
The AHF governance structure includes a Board of Directors whose responsibilities include final approval for the funding of healing projects, and an Executive Director that oversees the day to day management of the foundation. The AHF has been noted for excellence in governance and management. [Note 7]
The long term goal of the AHF has been to break the cycle of physical and sexual abuse that is a consequence of the legacy, and to create sustainable well-being for individuals and communities. The objective of the AHF is to address "the healing needs of Aboriginal People affected by the Legacy of Indian Residential Schools, including the intergenerational impacts, by supporting holistic and community-based healing to address needs of individuals, families and communities, including Communities of Interest". [Note 8] The activities and outputs of the AHF have included conferences and gatherings, training, research, the production of historical materials, and the promotion of awareness and understanding of the needs and issues surrounding residential school trauma and its legacy.
Community-based projects funded by the AHF were designed in and by communities to address the healing needs as understood by community members at the time; as a result, there is a range of healing approaches and modes used, within eight broad categories of eligible projects established by the AHF: (the last two of the list applied in the start-up phase):
- Those providing direct healing services;
- Those focused primarily on prevention of the effects of abuse, and awareness of the Legacy;
- Those that conduct Gatherings and conferences;
- Those that honour history by a variety of means, including memorials;
- Those focused primarily on training for potential healers and building capacity for the healing process;
- Those focused on knowledge-building, including through research and capacity building;
- Those focused on assessing the healing needs of the community (needs assessment); and
- Those that address project design and set-up.
The AHF model has emphasized a wholistic, community-based approach that emphasizes training and capacity building in healing; and reliance not only on "professional" healers, but healers with lived experience and cultural knowledge. One of the conclusions reached by AHF after several years of research, is that "culture is good medicine". [Note 9]
Projects are monitored by the AHF on the extent of their achievement of the following measures, intended to support the achievement of the overall program objective:
- Promotion of linkages to other government health and social services programs;
- Focus on early detection and prevention of the intergenerational impacts of physical and sexual abuse;
- Recognition of special needs, including those of the elderly, youth and women; and
- Promotion of capacity-building for communities to address their long-term healing needs. [Note 10]
Demand for AHF-funded projects in Aboriginal communities has been high; the AHF has received over $1.3 billion in funding requests since its inception, far outstripping the $515 million funding allocation. In 2001, there were 310 AHF-funded community projects, serving over 1,500 individual communities and approximately 60,000 individual participants. [Note 11] Currently, there are just over 140 contribution agreements for AHF projects distributed across the provinces and territories. Those projects that were funded under the 2007 endowment (i.e. 2007-2010 or 2012) are projects that have demonstrated ongoing success.
Table 1: Current Contribution Agreements by Region
| Region | Number of Contribution Agreements |
|---|---|
| Northwest Territories | 5 |
| Alberta | 10 |
| British Columbia | 19 |
| Manitoba | 27 |
| Labrador | 2 |
| Quebec | 19 |
| Nunavut | 12 |
| Yukon Territory | 4 |
| Ontario | 20 |
| Saskatchewan | 18 |
| New Brunswick | 2 |
| Nova Scotia | 2 |
| Prince Edward Island | 1 |
The final report of the Aboriginal Healing Foundation [Note 12] outlines the distribution of the Healing Fund by group, as follows: All groups (29%); Inuit (5%); Métis (5%); and First Nations (59%). In terms of distribution of projects by type, the majority have consistently been "direct healing" (e.g. therapy, counselling, on-the-land cultural-based activities), and the percentage of such programs has increased over time (59% in 2004; [Note 13] 65% in 2008 [Note 14]
2.0 Evaluation Methodology
2.1 Evaluation Scope and Timing
The evaluation covers the period from the implementation of the fund in April 2007 until May 2009, and the scope covers AHF community-based healing initiatives. Additionally, the evaluation addressed the question of the effectiveness of a foundation as a policy instrument to address Aboriginal healing needs; this was done primarily through a literature review and canvassing of expert opinion.
2.2 Objectives of the Evaluation
The overarching intent of the evaluation was to fulfill the requirement of Article 8.01(2) of the IRSS, which states that "Canada will conduct an evaluation of the healing initiatives and programmes undertaken by the Aboriginal Healing Foundation to determine the efficacy of such [healing] initiatives and programmes and recommend whether and to what extent funding should continue beyond the five year period". [Note 15]
As noted above, the primary objective of the evaluation has been to assess the efficacy of the healing initiatives and programs undertaken by the AHF under the Settlement Agreement for the period under review, and provide evidence that will support the government's decision-making regarding whether and to what extent funding should continue beyond the current end date of March 2010 for some projects and March 2012 for others (the 11 healing centres currently funded).
2.3 Evaluation Issues
The evaluation that was undertaken focused on the following broad issues:
- Whether and to what extent the expected outcomes were achieved;
- The impacts of the program (intended and unintended) on the healing needs of the target populations;
- To what extent the AHF is the best course for supporting healing initiatives;
- What possible alternatives there may be to the current program;
- The degree of cost-effectiveness of the projects;
- The implications of the terms and implementation of the funds on AHF project activity; and
- The need for such programs and government support for them (relevance).
The evaluation was guided by the following overarching themes and questions:
- Effectiveness and Success
- To what extent are Community-based healing initiatives meeting the needs of Aboriginal people affected by IRS?
- To what extent are Community-based healing initiatives meeting the needs of Aboriginal people affected by IRS?
- Impacts
- What have been the impacts (intended and unintended) of the healing programs?
- What have been the impacts (intended and unintended) of the healing programs?
- Relevance
- Is there a continued need for the programs and are they relevant to the needs?
- Is there a continued need for the programs and are they relevant to the needs?
- Cost-Effectiveness
- How does the cost of delivering AHF community-based healing programs compare to appropriate alternatives?
- How does the cost of delivering AHF community-based healing programs compare to appropriate alternatives?
- Other Evaluation Issues
- What options, alternatives, or changes could feasibly achieve the desired outcomes of AHF-funded programs?
- What options, alternatives, or changes could feasibly achieve the desired outcomes of AHF-funded programs?
2.4 Data Sources
Information used to inform the evaluation was gathered from multiple lines of evidence:
- Preliminary consultations with six subject experts;
- Review of 108 documents and literature sources;
- Review of Administrative files (Annual and quarterly reports for 07/08 and 08/09 for a sample of 29 AHF-funded projects (including the eight case study projects);
- 35 Key informant interviews of individuals from the following groups: AHF; relevant government departments; Aboriginal organizations; project directors from AHF-funded projects outside the case study sample; and subject experts from across Canada; and
- Eight Community case studies. (see Appendices for more detailed summaries of each)
- Case studies included a total of 145 interviews/group interviews with staff and other key stakeholders (n=72) and participants (n=73) at the following project sites:
- "Circle of Strength Youth Mental Health Healing Project" Keeseekoose First Nation, Yorkton, Saskatchewan (SK),
- "Healing Together Using Our Traditional Values and Ceremonies" Nunavik Regional Board of Health and Social Services, Kuujjuaq, Labrador,
- "Holistic Healing for Victims/Survivors of Shubenacadie School and their Descendants" Aboriginal Survivors for Healing, Charlottetown, Prince Edward Island (PEI),
- "Kisohkastwanaw – We are Resilient" Buffalo Lake Métis Settlement, Alberta (AB),
- "Mamisarqvik: A Healing Place" Tungasuvvingat Inuit, Ottawa, Ontario (ON),
- "The ‘Next Step' Process, Integrated Holistic Approach to Wellness and Changing the Legacy of Residential Schools", Eyaa-Keen Centre, Winnipeg, Manitoba (MB),
- First Nations House of Healing, "Tsa-Kwa-Luten Lodge" Inter Tribal Health Authority, Nanaimo, British Columbia (BC), and
- Yellowknives Dene First Nation Healing Project, Yellowknife, Northwest Territories (NWT).
- "Circle of Strength Youth Mental Health Healing Project" Keeseekoose First Nation, Yorkton, Saskatchewan (SK),
Interviews were conducted with program participants and key informants at case study sites as illustrated in Table 2, below. Case study key informants included project staff; frontline staff from other related community programs; traditional healers; and politicians.
Table 2: Case Study Interviews
| Case Study | Key Informants | Participant Surveys |
|---|---|---|
| "Healing Together", Kuujjuaq/Nunavik, Quebec | 7 | 7 |
| Tsa-Kwa-Luten Lodge, Inter-Tribal Health Authority, Nanaimo, BC | 30 | 11 |
| Mamisarqvik Healing Centre, Tungasuvvingat Inuit, Ottawa, ON | 10 | 5 |
| Yellowknives Dene First Nation Healing Project, Yellowknife, NWT | 6 | 5 |
| "Our Healing Journey", Buffalo Lake, AB | 11 | 6 |
| "Holistic Healing for Victims", Charlottetown, PEI | 9 | 9 |
| The "Next Step" Process, Eyaa-Keen Centre, Winnipeg, MB | 10 | 18 |
| "Circle of Strength", Keeseekoose, SK | 7 | 9 |
Case study sites were chosen according to a list of criteria to ensure that the sample represented all geographic regions; a range of urban, rural and semi-remote settings; all Aboriginal groups; and a range of project types, including healing centres.
The evaluation team consulted with an Advisory Group of AHF, government and independent experts who reviewed a Detailed Methodology Report and all data collection tools, as well as preliminary evaluation findings.
The evaluation methodology was adapted for this project to ensure cultural appropriateness of methods and the safety and wellbeing of participants. There were three primary ways of doing this: one was to provide for translation where needed to enable interviewees to participate in their Aboriginal language if desired; another was to design participant (i.e. Survivors and other project attendees) surveys so as to avoid causing any emotional harm; and finally, with the guidance and help of Health Canada, to arrange for Health Resolution Support Workers to be available for support to participants during and after they participated in the survey.
Case studies normally took place over a two-three day period, on-site at the project facilities [Note 16]
Of the program participants asked (n=66), 94 percent had either attended residential school or had a family member who attended. The age range of participants interviewed (n=72) is shown in the chart below.
Figure 1: Age Range of Participants (Case Study Surveys)

Figure 1: This figure shows a pie chart and legend, which groups the case study participants by age. There are four different age groups, each represented by a colour, and the chart shows the percentage representation for each group. It shows that 4% of participants were below the age of 25, 40% were between the ages of 25 and 45, 45% were between the ages of 45 and 60, and 11% were over the age of 60.
The gender breakdown of program participants interviewed for the evaluation was 63 percent female and 37 percent male.
2.5 Evaluation Limitations
Assessing Healing:
In strict terms, attribution of healing outcomes to specific program interventions is not possible in part, because of the following:
There here is no clearly defined or widely accepted agreement on what it means to be "healed" from the trauma of the residential school experience. Over the ten years of its mandate, the AHF has continually refined the list of indicators of healing that have been noted by project leaders and participants as meaningful to them; [Note 17] additionally, they have commissioned academic research on the meaning of healing with respect to the trauma of residential school. In the wider literature on this topic, the most recent scholarship is increasingly broadening the topic in two major ways: the roots of trauma are acknowledged to come from the entire colonization experience; [Note 18] and that these are enmeshed with the IRS experience; and trauma is acknowledged as going far beyond the individual, broadening the concept of healing beyond individuals to families, social networks and communities as a whole.
Healing is a long-term, complex, and non-linear process that is difficult to evaluate at any one period in time. [Note 19] Accordingly, the conclusions of the evaluation come from many lines of evidence in addition to the primary research undertaken: selected documents representing the ten years of evaluation and research undertaken by the AHF, including the three-volume Final Report; other relevant literature on Aboriginal trauma and healing and evaluation of these; and AHF reports from a sample of projects for the years 2007-2009.
It is recognized that wider social indicators (e.g. crime rates, poverty, suicide rates, education levels, physical health) have a direct impact on an individual's ability to achieve and maintain healing, but no accurate recent data are available on such indicators for Aboriginal communities. Without such a baseline, it is not possible to chart the extent to which communities may or may not be "healing" in these areas. The evidence for such indicators presented in this evaluation is based principally on the knowledge and experience of interviewees.
- The evaluation took place over a short time period and during the summer months, when it is difficult to contact interviewees.
- Over the time period under review, the client population changed. While some participants enrolled in programs more than once, programs were continually enrolling new participants, and therefore, data over the time period does not reflect the same target group.
- The Case study data are analyzed together as one sample, but represent a very diverse set of circumstances, from large healing centres to a small project with one staff member, and include Inuit, Métis and First Nations projects, which differ in some key aspects.
- With respect to in-depth analysis of case-study findings and Quarterly reports, differences in reported participation rates were a data limitation.
- A lack of costs data per project per fiscal year within Annual Reports; a shortage of program delivery costs in general, and a lack of any true comparators, inhibit the ability to make a cost effectiveness analysis.
- Aboriginal healing of IRS effects is a highly specialized area, and there is limited research available for comparative purposes and best practice knowledge.
- The nature of project file data (i.e. the sample of 29 projects reviewed) in some cases made analysis difficult, due to what evaluators perceived as possible confusion on the part of project reporters regarding whether to report an indicator as "emerging" or "established"; [Note 20] In some cases, indicators were reported as both [Note 21] and notes attached to reports indicated that this was done because both appeared to be the case. Furthermore, because of the diverse nature of projects; the fact that not all are community based, and some serve a number of communities; reporting whether indicators are "emerging" or "established" in some cases would be extremely challenging for project reporters. For example, in the case where one project serves a number of communities; an indicator may be established in one of the communities but not in others; [Note 22]
- Participants were a targeted, and not a random sample. Due in large part to the severe time constraints of the evaluation, participants were selected by case study sites themselves, rather than chosen randomly by evaluators.
- With respect to in-depth analysis of case-study findings and Quarterly reports, differences in reported participation rates were a data limitation.
Effects of Evaluation on people who have suffered IRS-related trauma
A concern at the outset of the evaluation was the need to protect the safety of program participants who would be taking part, including some program staff who are also Survivors of residential school. The evaluation team found this concern to be well-founded, as we conducted interviews with Survivors. The experience of talking about the topic, even without direct questions regarding IRS experiences, was very difficult for many participants. Health Canada's Health Resolution Support Workers or on-site counselors were ready to de-brief and counsel those who were affected in this way. Although the need for such safety and support is well understood by AHF and Health Canada, it bears reiteration here for evaluators and other researchers, and has clear implications for the ongoing Common Experience Payment (CEP), Independent Assessment Process (IAP) and Truth and Reconciliation Commission (TRC) processes.
Attributes of Outcomes To Program Activities
Accurate assessment of the impacts and outcomes of a community-based social program is recognized in the literature as "usually not possible, even with a carefully designed evaluation study." [Note 23] A more achievable goal is to present evidence that will improve our understanding of the difference made by the program, or its contribution, and to present multiple lines of evidence that speak to program effectiveness. In this evaluation, certainty of attribution of outcomes to program activities is not possible by strict evaluation standards; however, there is a high degree of consistency in the data collected, which increases confidence in the findings.
3.0 Evaluation Findings
3.1 Effectiveness and Success
Background:
Surveys conducted by AHF in 2000, 2002, and 2004 cite an estimated 204,564 participants in AHF-funded healing projects, two-thirds of which had not previously participated in similar activities. [Note 24] The same surveys document an estimated 49,095 individuals who participated in AHF-funded training projects.
In terms of achieving healing outcomes, the AHF Final Report estimated in 2006 that 20 percent of the communities who participated were just beginning healing activities; 65.9 percent of the communities had accomplished some goals, but needed much more work; and 14.1 percent of the communities accomplished many goals. A project goal seen by the AHF as a "pivotal first step to the eventual success of healing endeavours" [Note 25] is the raising of awareness of the history and effects of IRS.
Indicators of Effectiveness and Success:
Over the ten years of its mandate, AHF has refined the understanding of what Survivors, healers and communities understand as indicators of healing of IRS effects. The evaluation used this accumulated knowledge as a guide in selecting indicators of effectiveness and success as areas of investigation for the evaluation.
Accordingly, the level of awareness of IRS and its effects; participation rates and changes in these; the percentage of attendees who are participating in healing for the first time; the degree to which specific needs are being addressed (e.g. youth, elderly, men) the levels of disclosure of abuse; increases in sobriety; the level of support for projects by community leaders; the level of volunteerism supporting projects; the degree to which projects have engaged other service providers and funders for sustainability; time-tested indicators of how effective projects have been at addressing healing needs as defined by communities, were used.
Findings presented below include data from a review of project files for 29 community-based projects, interviews at case study sites, and key informant interviews. The guiding evaluation question was: "To what extent are community-based healing initiatives meeting the healing needs of Aboriginal people affected by Indian Residential Schools?" Some of the charts presented below show less than 29 projects; in these cases, that particular indicator was not reported on for a small number of projects. In cases where the number exceeds 29, projects reported one indicator as both "established" and "emerging" (see note above in Section 2.5).Results are not always unambiguous, due to reporting requirements, as discussed above; for example, the ranking of some indicators as "emerging" may have grown, while that indicator's status as "established" may have decreased over the time period. There are a number of possible explanations for this:
- Project enrolment is growing, which in many cases means that people who are just beginning their healing may outnumber those who are well along in the process; therefore, the assessment of an indicator as "established" will go down, and will rise as "emerging";
- The trajectory of healing is non-linear and long term; the plotting of levels of sobriety, for instance, would be a jagged, rather than a straight line;
- The annual reports assume a community-based project where reporters can report on community conditions. In a number of cases, projects are either based in large urban areas; take clients from across the country; or serve a number of communities with different characteristics. In these cases, reporters would find it difficult to fit their data to the reporting format;
- As the AHF has learned, project success is intimately linked with community dynamics, and factors such as change in community leadership can have major effects on community-level indicators such as volunteerism; and
- A rise in disclosure of sexual abuse would be a positive indicator from the perspective of individuals and families taking the first step towards healing; however, the initial stages following disclosure can also have negative effects on family and community relations that might be reflected in assessments of community conditions.
Intuitively, the reader may feel that a decrease in "established" ranking of an indicator is a negative sign. Evaluators did not make this assessment in most cases, based on the overall findings which show such a dramatic rise in program enrolments (over 40 percent), and the overwhelmingly positive assessment of AHF programs by participants and key informants in communities (some of whom were not directly connected to the program).
Project File Review shows the following:
Projects report that awareness levels are fairly established, both in youth participation/interest as well as Legacy awareness; healing capacity is established in most communities. Indicators of healing such as sobriety, disclosure and other community capacity indicators (i.e. volunteerism) are still emerging. Of 29 projects reviewed, 27.6 percent of projects (n=8 of 29) reported more than half of community healing indicators in 2008/09 as "established".
Program enrolment is growing:
Participation from 2007/08 to 2008/09 increased by 40 percent (7,899 more reported participants in all programs), but case study interviewees noted this was done with no increase in funding or other resources. In 2007/08, 19,642 participants were reported in all programs (for 28 projects), 40 percent of which (7,733) were attending a project activity for the first time. In 2008/09, 27,541 participants were reported in all programs (for 28 projects); 25 percent (6,913) of these participants were attending a project activity for the first time; 11 percent fewer people were listed as a new attendee in 2008/09 than 2007/08.
Figure 2: Number of Participants 2007-08

Figure 2: This figure shows a pie chart indicating the number of participants for all AHF programs in 2007-08. It shows that in that year, 61% of participants were repeat attendees and 39% were first time attendees.
Figure 3: Number of Participants 2008-09
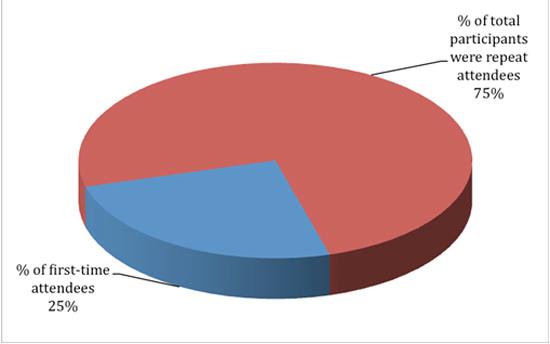
Figure 3: This figure shows a pie chart indicating the number of participants for all AHF programs in 2008-09. It shows that in that year, 75% of participants were repeat attendees and 25% were first time attendees.
Participation by Target Group and Gender Participation:
A file review for case study sites [Note 26] shows that the majority of program participants are women. This is consistent with normal patterns in Aboriginal communities, where men are known to be a hard-to-reach target group for healing. Given this, the levels of reach to men as a target group for some of the programs (almost 50 percent in some cases) can be taken as an indication of success.
Figure 4: 4th Quarter 2007-08 Gender Participation (Case Studies)
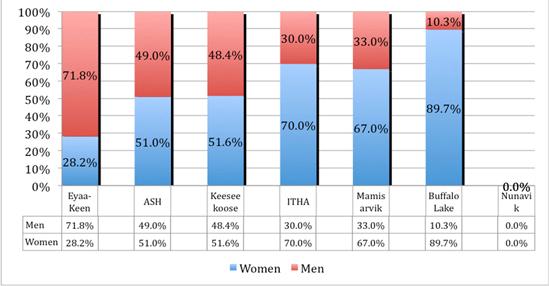
Figure 4: This figure shows a graph which groups the case study participants for the fourth quarter of 2007-08 by gender. Each gender is represented by a different coloured portion of the bars on the graph.
The graph shows that in Eyaa Keen, 28.2% of participants were women and 71.8% were men; in ASH, 51.0% of participants were women and 49.0% were men; in Keeseekoose, 51.6% of participants were women and 48.4% were men; in ITHA, 70.0% of participants were women and 30.0% were men; in Mamisarvik, 67.0% of participants were women and 33.0% were men; and in Buffalo Lake, 89.7% of participants were women and 10.3% of participants were men. Data is not available for the Nunavik case study for 2007-08.
Figure 5: 4th Quarter 2008-09 Gender Participation (Case Studies)
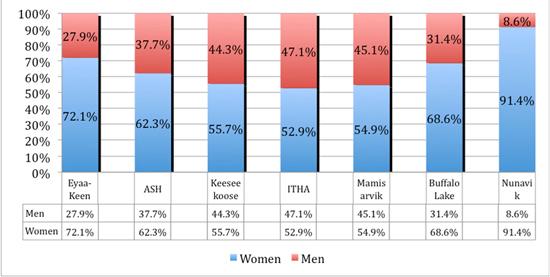
Figure 5: This figure shows a graph which groups the case study participants for the fourth quarter of 2008-09 by gender. Each gender is represented by a different coloured portion of the bars on the graph.
The graph shows that in Eyaa Keen, 72.1% of participants were women and 27.9% were men; in ASH, 62.3% of participants were women and 37.7% were men; in Keeseekoose, 55.7% of participants were women and 44.3% were men; in ITHA, 52.9% of participants were women and 47.1% were men; in Mamisarvik, 54.9% of participants were women and 45.1% were men; in Buffalo Lake, 68.6% of participants were women and 31.4% were men; and in Nunavik, 91.4% of participants were women and 8.6% of participants were men.
File review for the sample of 29 projects shows that in 2007/08, 66.7 percent of projects (n=18 of 27) reported that participation in healing projects by specific groups was an established indicator, and 18.5 percent (n=5 of 27) reported this as "emerging". In 2008/09, 57.1 percent of projects (n=16 of 28) reported participation by specific target groups was established, and 32.1 percent of projects (n=9 of 28) reported as "emerging". The percentage of those reporting no participation by target groups dropped from 14.8 percent (n=4 of 27) in 2007/08 to 10.8 percent in 2008/09, indicating that target groups (such as men, youth, Elders) are increasingly being reached.
Participation of Survivors in healing activities:
"Survivors", or those who attended residential schools, were the main focus of early healing efforts by projects; over the years, an understanding has emerged that the IRS effects on these individuals was passed on through families and wider social networks. Interviewees noted that Survivors are often reluctant to come out from the refuge of secrecy and the burden of shame to reveal their experiences of abuse and trauma; therefore, the degree of Survivor participation is used as a measure of the effectiveness of healing programs.
Survivor participation is growing:
File review shows that 51.8 percent of projects (n=14 of 27) reported local Survivors involved in awareness-raising activities as an emerging activity; this is an increase of 40 percent over the 2007/08 period.
Figures 6 and 7, below, illustrate survivor participation rates for the case study sites. [Note 27] It is clear that, in most of these projects, Survivors are the minority of project participants. Factors influencing this rate would include the numbers of Survivors in the community; the historical pattern of residential school attendance that would affect the age of Survivors in that particular site; and the particular type of program offered. It was also noted by case study key respondents that there are few actual Survivors remaining, but that the IRS effects have radiated far beyond those individuals.
Figure 6: 4th Quarter 2007-08 Survivor Participation (Case Studies)
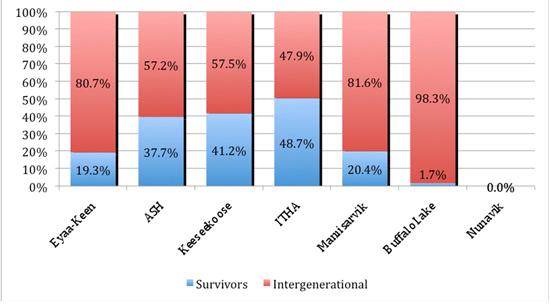
Figure 6: This figure shows a graph indicating the rates of IRS Survivor participation in case study groups for the fourth quarter of 2007-08. Survivors and Intergenerational participants are each represented by a different coloured portion of the bars on the graph.
The graph shows that in Eyaa-Keen,19.3% of participants were Survivors and 80.7% were Intergenerational; in ASH, 37.7% of participants were Survivors and 57.2% were Intergenerational; in Keeseekoose, 41.2% of participants were Survivors and 57.5% were Intergenerational; in ITHA, 48.7% of participants were Survivors and 47.9% were Intergenerational; in Mamisarvik, 20.4% of participants were Survivors and 81.6% were Intergenerational; and in Buffalo Lake, 1.7% of participants were Survivors and 98.3% were Intergenerational. Data is not available for the Nunavik case study for 2007-08.
Figure 7: 4th Quarter 2008-09 Survivor Participation (Case Studies)

Figure 7: This figure shows a graph indicating the rates of IRS Survivor participation in case study groups for the fourth quarter of 2008-09. Survivors and Intergenerational participants are each represented by a different coloured portion of the bars on the graph.
The graph shows that in Eyaa-Keen, 66.5% of participants were Survivors and 33.5% were Intergenerational; in ASH, 39.6% of participants were Survivors and 60.0% were Intergenerational; in Keeseekoose, 53.2% of participants were Survivors and 44.2% were Intergenerational; in ITHA, 24.2% of participants were Survivors and 50.3% were Intergenerational; in Mamisarvik, 32.3% of participants were Survivors and 44.2% were Intergenerational; in Buffalo Lake, 1.4% of participants were Survivors and 98.6% were Intergenerational; and in Nunavik, 10.0% of participants were Survivors and 90.0% were Intergenerational.
As noted above, AHF has learned that awareness-raising activities are a "pivotal first step" in the healing process. Interviewees noted that once the knowledge of IRS effects on attendees becomes known, the climate is created for disclosure and the beginning of healing, and family members gain an understanding not only of a major part of their history, but of the behaviour patterns of Survivors. Awareness-raising activities are increasing; in 2008/09, 77.8 percent of projects did such activities, a higher rate than the previous year. Most projects (70.8 percent) in 2008/09 reported including Survivors and their families as an established part of healing.
Evidence of Effectiveness and Success from Participant Surveys:
When asked to rate the effectiveness of healing projects, 62 percent of respondents noted that the programs had contributed to their healing either "quite a bit" or that "most of" their healing had come through attendance at the program., (as Figure 8, below, illustrates.)
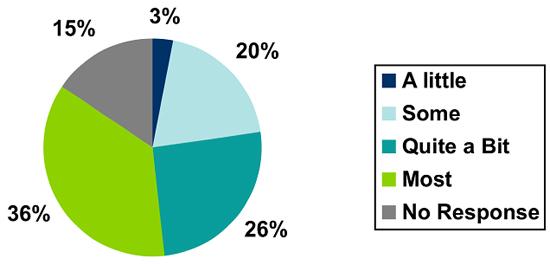
Figure 8: This figure shows a pie chart demonstrating the effectiveness of healing projects based on the response of participant surveys to the question, "How much has this project helped you on your healing journey?". 36% of respondents indicated "most" of their healing had come through program attendance; 26% of respondents indicated "quite a bit"; 20% of respondents indicated "some"; 3% of respondents indicated "a little" and 15% of participant surveys indicated "no response".
As an indicator of the effectiveness of programs to connect to other types of healing, program participants were asked the extent to which the AHF program had helped them connect to other types of healing (e.g. rehab, psychotherapy, other counselling), 53 percent of program participant respondents said that the healing program had helped them connect to other kinds of healing required to address the effects of IRS. (See Figure 9, below)
9: Response to "Has this program ever helped you to connect with other kinds of healing you need because of the legacy of residential school?"
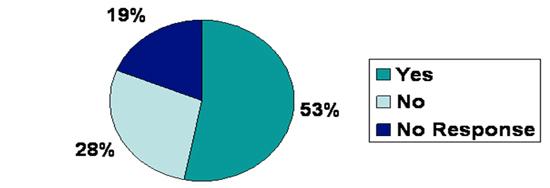
Figure 9: This figure shows a pie chart demonstrating the effectiveness of programs to connect to other types of healing based on the response of participant surveys to the question, "Has this program ever helped you to connect with other kinds of healing you need because of the legacy of residential school?". 53% of respondents indicated "yes", 28% of respondents indicated "no", and 19% of survey participants indicated "no response".
Many of those who replied "no" qualified this answer by noting that there were no other accessible healing alternatives available for this specific type of healing. This lack of healing alternatives comparable to AHF healing programs was reiterated by project managers and key informants in interviews.
3.1.1 Building Capacity
Another indicator used to measure effectiveness and success is the degree to which capacity has been built in communities, either through training of healers or engagement of volunteers, particularly Survivors. The building of social capital (of which volunteerism is a part) is recognized by AHF and in the wider literature as a critical component of individual and community healing. One component of this of particular importance in Aboriginal communities is the engagement of Youth, both with their cultural heritage and with Elders. Their degree of engagement is also recognized as an indicator of community capacity.Figure 10: Community indicator - Youth are interested in learning about Aboriginal culture, language and history
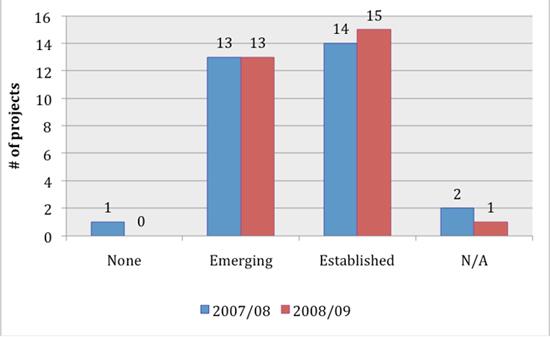
Figure 10: This figure shows a graph illustrating aboriginal youth engagement with cultural heritage as an indicator of community capacity in AHF projects. Data collected for the years 2007-08 is represented by one colour on the graph and data collected for the years 2008-09 is represented by another. In 2007-08, one project reported that youth were not engaged; thirteen projects reported an emerging engagement; fourteen projects reported an established engagement and two projects reported that the trend was not applicable to them. In 2008-09, none of the projects reported that there was no youth engagement; thirteen projects reported an emerging engagement; fifteen projects reported an established engagement and one project reported that the trend was not applicable to them.
File review shows that the building of strong teams of leaders with a variety of skills is firmly established in the majority of projects (n=29), as illustrated in the graph below.
Figure 11: Community indicator - Community has a strong, dedicated healing team

Figure 11: This figure shows a graph illustrating community capacity in AHF projects in terms of building a strong, dedicated healing team with a variety of skills. Data collected for the years 2007-08 is represented by one colour and data collected for the years 2008-09 is represented by another. In 2007-08, none of the projects indicated that there was no dedicated healing team with a variety of skills; nine projects indicated a team was emerging and twenty-one projects indicated a team was established. In 2008-09, one AHF project indicated that there was no dedicated healing team with a variety of skills; six projects indicated a team was emerging and twenty-two projects indicated a team was established.
While capacity in volunteerism is growing, this indicator is reported to be more in the "emerging" stage than "established"; Volunteerism was reported as "emerging" by 41.4 percent of projects (n=12 of 29 [Note 28]) in 2007/08; this increased to 57.1 percent of projects (n=16 of 28 [Note 29]) in 2008/09. Volunteerism was reported as established by 41.4 percent of projects (n=12 of 29) in 2007/08; but by 32.1 percent of projects (n=9 of 28) in 2008/09. Overall, the number of projects with some volunteering remained relatively stable with 24 in 2007/08 and 25 in 2008/09. The projects reporting no volunteering at all had decreased over the period.
Survivors moving from wanting help to helping others was reported as "emerging" by 66 percent of projects (n=29) in both years.
Figure 12: Community indicator - People are volunteering
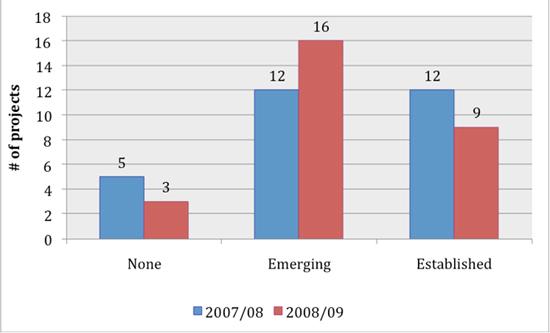
Figure 12: This figure shows a graph illustrating volunteerism as a community capacity indicator in sample AHF projects. Data collected for the years 2007-08 is represented by one colour on the graph and data collected for the years 2008-09 is represented by another. In 2007-08, five projects reported that volunteerism was not an established trend; twelve projects reported an emerging trend of volunteerism and twelve projects reported that volunteerism was established. In 2008-09, three projects reported that volunteerism was not an established trend, sixteen projects reported an emerging trend of volunteerism and nine projects reported that volunteerism was established.
The degree of informal help offered between individual and families within communities is another indicator of community capacity for healing; this is reportedly increasing. Figure 13, below shows that in 2007/08, 23 percent of projects (n=7 of 29) reported helping others as established, and this number increased to 31 percent of projects (n=9 of 29) in 2008/09.
Figure 13: Informal Help as an Indicator of Community Capacity

Figure 13: This figure shows a graph that illustrates Survivor volunteerism in sample AHF projects. Data collected for the years 2007-08 is represented by one colour on the graph and data collected for the years 2008-09 is represented by another. In 2007-08, three projects reported that there was no trend of Survivors volunteering; twenty projects reported an emerging trend of Survivor volunteerism and seven projects reported an established trend of Survivor volunteerism. In 2008-09, one project reported that there was no trend of Survivors volunteering; nineteen projects reported an emerging trend of Survivor volunteerism and nine projects reported an established trend of Survivor volunteerism.
Community involvement and help in general is reported as established by the majority of projects; Figure 14, below, illustrates that 63.3 percent of projects (n=19 of 30 [Note 30]) reported that people are socializing, visiting Elders, and actively contributing to community events. The reported number decreased slightly to 58.6 percent (n=17 of 29) of in 2008/09.
Figure 14: Community indicator – People are socializing, visiting Elders and actively contributing to community events
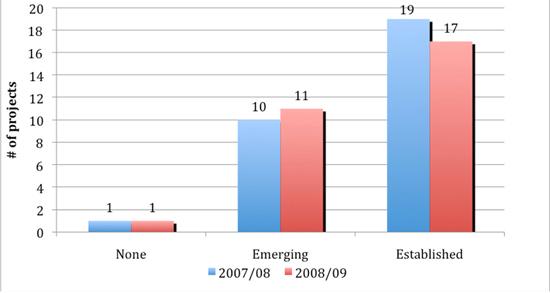
Figure 14: This figure shows a graph illustrating community involvement as an indicator of healing capacity in sample AHF project communities. Data collected for the years 2007-08 is represented by one colour on the graph and data collected for the years 2008-09 is represented by another. In 2007-08, one project reported no community involvement; ten projects reported emerging community involvement and nineteen projects reported established community involvement. In 2008-09, one project reported no community involvement; eleven projects reported emerging community involvement and seventeen projects reported established community involvement.
Leadership support appears to be growing:
Another indicator of the degree of capacity for healing in communities is the extent of support and engagement by community leaders. As would be expected, support is more robust than active engagement in projects; however, both indicators show increasing support by community leaders. File review showed that all but one project reported support from community leaders either emerging or established; in terms of participation, 72.4 percent of projects (n=21 of 29) reported participation by community leaders as emerging or established in 07/08, which increased to 83.3 percent (n=25 of 30 [Note 31]) in 08/09. The ranking of this indicator would be sensitive over time to changes in community leadership.
Figure 15: Community indicator – "Community leaders support healing"

Figure 15: This figure shows a graph indicating the healing support community leaders provide in sample AHF project communities. Data collected for the years 2007-08 is represented by one colour and data collected for the years 2008-09 is represented by another. In 2007-08, one project reported that there was no community leaders' support for healing; twelve projects reported an emerging trend of community leaders' support and sixteen projects reported community leaders' support was established. In 2008-09, one project reported that there was no community leaders' support for healing; fourteen projects reported an emerging trend of community leaders' support and fourteen projects reported that community leaders' support was established.
Figure 16: Community indicator – "Community leaders participate in healing"
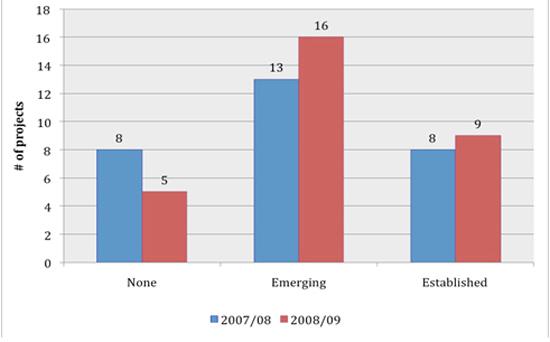
Figure 16: This figure shows a graph illustrating community leaders' participation in healing in sample AHF project communities. Data collected for the years 2007-08 is represented by one colour and data collected for the years 2008-09 is represented by another. In 2007-08, eight projects reported that there was no community leaders' participation in healing; thirteen projects reported an emerging trend of community leaders' participation and eight projects reported that community leaders' participation was established. In 2008-09, five projects reported that there was no community leaders' participation in healing; sixteen projects reported an emerging trend of community leaders' participation and nine projects reported that community leaders' participation was established.
3.1.2 Achieving Healing Outcomes
Indicators used to determine the extent to which programs are achieving healing outcomes include: people speaking openly about their IRS experiences (which is acknowledged as a critical first step in healing); community awareness of the history of residential schools and their effects on individuals and families; the extent to which levels of sobriety have changed in communities.
As Figure 17 below illustrates, file review of these selected indicators shows that the majority of the sampled projects (n=29) report this as an established indicator for their community, and that this has grown between 2007/08 and 2008/09. Disclosure of Residential School experiences is generally reported to be increasing. 54.8 percent of projects (n=17 of 31 [Note 32]) reported that disclosure was established in 2008/09, compared to 46.7 percent (n=14 of 30 [Note 33]) in 2007/08.
Figure 17: Community indicator – People speak openly about their Residential School experiences
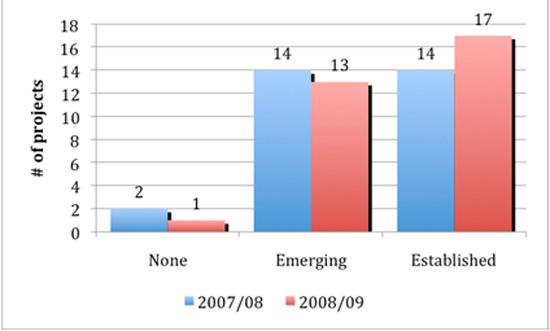
Figure 17: This figure shows a graph illustrating healing outcomes in terms of people speaking openly about their IRS experience in sample AHF projects. Data collected for the years 2007-08 is represented by one colour and data collected for the years 2008-09 is represented by another. In 2007-08, two sample projects reported that there was no trend of people speaking openly about their IRS experiences, fourteen projects reported an emerging trend and fourteen projects reported an established trend. In 2008-09, one sample project reported that there was no trend of people speaking openly about their IRS experiences, thirteen projects reported an emerging trend and seventeen projects reported an established trend.
While all programs report that participants are familiar to some degree with Residential Schools and their community history; the number reporting this as "established" went down from 72.4 percent (n-21 of 29) in 2007/08 to 59 percent (n=17 of 29) in 2008/09.
Figure 18: Community indicator – People are familiar with the Legacy and history of their community

Figure 18: This figure shows a graph indicating awareness of the IRS experience and history within sample AHF project communities. Data collected for the years 2007-08 is represented by one colour and data collected for the years 2008-09 is represented by another. In 2007-08, eight projects reported an emerging trend of community awareness and twenty-one projects reported an established trend. In 2008-09, twelve projects reported an emerging trend of community awareness and seventeen projects reported an established trend.
As addictions are closely linked to IRS trauma, increased sobriety in a community is recognized as an indicator of progress in healing. Project files show that the majority of projects in the sample report this as an "emerging" indicator, and that the percentage of projects reporting this increased to some extent between 2007/08 and 2008/09. (see Figure 19, below)
Figure 19: Community indicator – Increased sobriety in the community
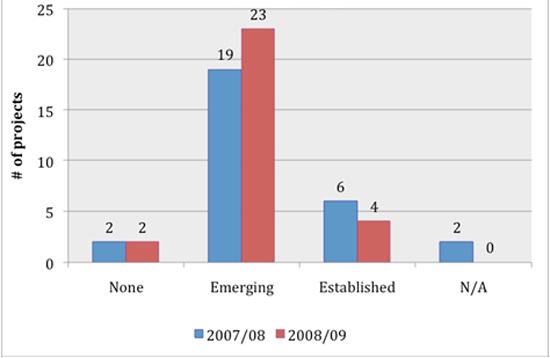
Figure 19: This figure shows a graph indicating the extent to which levels of sobriety have changed in AHF project communities. Data collected for the years 2007-08 is represented by one colour and data collected for the years 2008-09 is represented by another. In 2007-08, two projects reported that there was no increase in sobriety, nineteen projects reported an emerging trend of increased sobriety, six projects reported an established trend, and two projects reported that the trend was not applicable to them. In 2008-09, two projects reported that there was no increase in sobriety, twenty-three projects reported an emerging trend of increased sobriety, and four projects reported an established trend.
There were particular instances of success noted in the literature and interviews with key informants. One of these is Mamisarvik Healing Centre, an Inuit-focused project in Ottawa, which uses a screening tool on intake. Analysis of that data indicated the presence of Post-traumatic Stress Disorder (PTSD) in approximately 85 percent of clients. Following eight weeks of treatment, the indicators for PTSD are "significantly reduced or gone for most". [Note 34]
A number of interviewees reported their knowledge of decreases in suicide rates and child apprehensions, and increases in intergenerational communication and interaction, particularly between Elders and youth, as a result of AHF healing programs. A program in Saskatchewan reported successfully rehabilitating an individual in his 50's, an IRS attendee for many years who was sexually abused, who had been incarcerated for most of his adult life, including for sex offences. [Note 35]
3.1.3 Challenges to Administration and Delivery
Challenges to program administration and delivery noted by Key Respondents (case study participants, including: program boards, directors, healers and other staff; and other key respondents such as experts) include the following:
- Funding: both a shortage of funds in the face of rising enrolments and increased demand for services, and the challenge (over the entire funding period) of uncertainty of funding. This was by far the most cited challenge by case study interviewees. One of the aspects of this that is affecting current projects, including those in the case study sample, is the impending closure of all but the healing centres in March 2010; (the healing centres receive operational funding and will continue until March 2012). Interviewees noted that the uncertainty of the winding-down period makes it difficult to retain staff;
- Staffing: Projects have found it difficult to attract qualified staff, both those trained in mainstream healing modes, and Aboriginal cultural experts/healers;
- Training: Respondents note that there have not been enough training opportunities for existing staff to build healing capacity to required levels within communities. In particular, staff report being challenged by complex healing needs and crisis situations. The same challenge was noted in the AHF Final Report (Vol. 1, p. 171), which noted the consistent requests from project staff for "targeted, advanced training to meet the needs";
- Reports indicate that the increased demand for project services is due, at least in part by, the CEP, IAP andTRC, both by triggering disclosure and the seeking of healing by more Survivors, and by demands on projects for assistance in navigating the CEP and/or IAP processes. As a result, projects have reported an increase in demand for their services without an increase in funding or staffing; in some cases, healing services have been pre-empted by the immediate demands of Survivors needing assistance withCEP/IAP processes (see Section 3.2.2, below, for a more detailed discussion of this). It was noted by some respondents that clients state their preference for AHF programs over government programs, because it is an Aboriginal organization, which they can trust; [Note 36]
- Travel and childcare costs prohibit participation of some potential participants (the scale of this challenge differs according to urban or rural location of project);
- Community determinants of health (i.e. social indicators) remain challenging: (e.g.. poverty, housing conditions, family violence, addictions, sexual abuse, suicide and grief); there is still a high level of need for healing. Many interviewees remarked that the needs that have been addressed are "just the tip of the iceberg";
- Limited support from leadership in some cases: while projects file review noted this was improving, it was reported as a challenge in some case study sites;
- Project staff are strained by project demands, with little time to devote to seeking outside resources;
- Different cultural approaches regarding models of healing that should be employed (e.g. Medicine Wheel);
- Limited alternative healing resources in community context for referral of complex needs clients;
- There are limited resources for follow-up care of program clients;
- Religious opposition in some communities to healing activities;
- There is a need for more Inuit-specific services;
- Inuit projects were started later than others; hence the healing period for Inuit Survivors has been shorter; and
- Inuit projects are challenged by the reality of much higher costs in the North.
Challenges noted in previous evaluations conducted by the AHF (Kishk Anaquot Health Research 2001, 2002, 2003), include fear, denial and resistance; and the challenge of engaging men in programs. It is notable that these challenges are rarely mentioned now, and serves as an indication of the progress that has been achieved in these areas, in terms of raising awareness and reaching out to men, a target group notoriously difficult to reach.
Resistance and opposition to healing programs within communities are seldom cited now as challenges, indicating an improvement in this indicator of community capacity.
3.1.4 Sustainability of Initiatives
Background:
Linkages and partnerships, particularly funding agreements, were selected as key indicators of project sustainability. The Funding Agreement stipulates that "In order to be eligible, projects…shall establish complementary linkages, where possible in the opinion of the Board, to other health/social programs and services (federal / provincial / territorial / Aboriginal)" (AHF Funding Agreement 2007). National survey results show that 85 percent of projects were addressing the legacy of residential schools in collaboration with other agencies or organizations (Degagné 2008).
Partnerships and linkages:
Review of the selected sample of project files for the two years (n=29) shows that:
- In 2007/08, 38 percent of projects reported having no partner funding of any type; this had increased to 45 percent in the following year.
- The majority of projects have partner funding support of less than $10,000 per year.
- Roughly $1.4 million of support was reported in 2007/08, and just over $1.8 million in 2008/09; however, over $850,000 was from a single contribution to one program. Just over $950,000 was reported in total funding partnerships for the 28 others, a decrease of over $450,000.
Figure20: Partnership support to projects by year
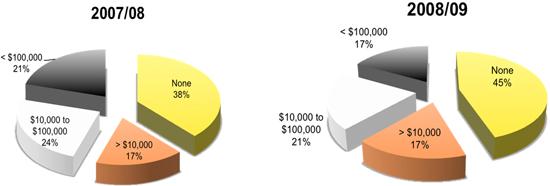
Figure 20: This figure shows two pie charts which indicate levels of funding support from Partnerships in sample AHF projects. There are four different funding level groups, each represented by a colour, and the charts show the percentage representation for each group. The first chart illustrates data collected for the year 2007-08. The chart shows that 38% of the sample projects received no Partnership funding, 17% received less than $10 000, 24% received between $10 000 and $100 000, and 21% received more than $100 000. The second chart illustrates data collected for the year 2007-08. The chart shows that 45% of the sample projects received no Partnership funding, 17% received less than $10 000, 21% received between $10 000 and $100 000, and 17% received more than $100 000.
- Other partnership initiatives included private charity linkages, Legacy of Hope and other IRS support organizations, municipal support, and justice agencies support.
- Many projects listed partnerships with other agencies but provided no details on in-kind funding; these were primarily described as cross-referrals, collaborative programming, or services/expertise the AHF project provided to other agencies.
- Health, Education and Addictions agency partnerships were the most commonly cited linkages.
Figure 21: Identified Partnerships by Type, 2007-08
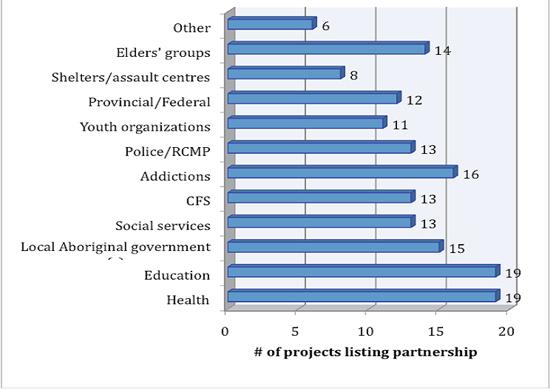
Figure 21: This figure shows a graph indentifying the types of Partnerships made with AHF projects in 2007-08. There are twelve types of Partnerships listed and the graph shows the number of projects listing each type of Partnership. The projects cited types of Partnerships as follows: Nineteen projects claimed Partnership with health organizations; nineteen with organizations related to education; fifteen with local aboriginal government; thirteen with social services; thirteen with CFS; sixteen with addictions organizations; thirteen with the police/RCMP.; eleven with youth organizations; twelve with provincial/federal governments; eight with shelters/assault centres; fourteen with Elders' groups and six with other types of organizations.
Linkages and Cross-referrals:
In both 07/08 and 08/09, slightly more than half of projects whose files were reviewed (51.9 percent or n=14 of 27 [Note 37] projects and 51.7 percent or n=15 of 29 projects respectively) reported referrals from mainstream services to community based healing initiatives as "established". Mainstream services and agencies include those at all levels, including local municipal, regional Aboriginal provincial/territorial organizations; Survivor organizations, provincial and federal government departments.
Figure 22: Community Indicator – Referrals from Mainstream Services
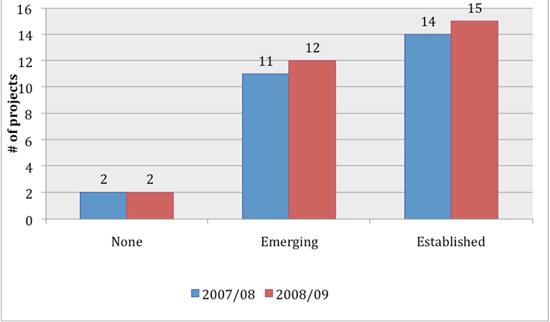
Figure 22: This figure shows a graph indicating trends in referrals from mainstream services to community-based healing initiatives in AHF projects. Data collected for the years 2007-08 is represented by one colour and data collected for the years 2008-09 is represented by another. In 2007-08, two projects reported that there were no referrals from mainstream services; eleven projects reported an emerging trend in referrals and fourteen projects reported an established trend in referrals. In 2008-09, two projects reported that there were no referrals from mainstream services; twelve projects reported an emerging trend in referrals and fifteen projects reported an established trend in referrals.
Case study findings are that while linkages for cross-referrals and some sharing of resources is common amongst the case studies, most projects have limited resources for continued funding; in part because there are few, if any, agencies with a matching mandate as suitable partners. As a result, many projects are sustainable from the point of view of continued need and supportive referral environments to existing (although limited) resources, but not in terms of funding. A number of the case study projects reported receiving referrals from mainstream service providers such as mental health counselors and social workers; for example, the First Nations House of Healing on Vancouver Island showed a 65 percent increase in referrals from other agencies in the period under review.
Interviewees noted also that Aboriginal clients prefer AHF healing programs to government and other mainstream services because they are perceived as offering Aboriginal services in a culturally safe environment, and that they are entitled to such a choice.
3.2 Impacts
3.2.1 Program Impacts
Case study interviews provided the following information on the reported impacts of healing projects; these were reported by program participants, staff/healers, community leaders, and frontline workers in communities and partner agencies.
- Learning to take action and responsibility for one's own health and healing was the most often cited impact by program participants;
- Increased community capacity for healing as indicated by increased awareness; decrease in anger and resistance to healing initiatives; "healing" is now an acknowledged and better understood concept. Interviewees who were family members of Survivors noted that, by learning the history of IRS and its impacts, they for the first time understood the Survivors in their family. Increased awareness was the second most-often mentioned impact of healing programs by program participants in case study interviews, and this was linked to changed attitudes towards family members (particularly Survivors);
- Increase in cultural knowledge, decreased shame in Aboriginal identity and increased pride and celebration of culture. Many respondents cited the learning or re-connection with their culture as the key to a recovered sense of self and one's place in the world, from which a number of positive actions could flow;
- Increased pride and self-esteem has led to achievements in education and work life for many participants;
- Reported healing of trauma and negative emotions and the acquisition of "tools" for continuance of self-care in this area; one mental health expert's description of this approach was to say that "healing is a key precondition for people [who have been institutionalized and therefore dependent] to find their pathway to self-care";
- Reported decrease in sense of isolation through realization and sharing of many similar stories of IRS effects; programs seen as a "safe place" to disclose experiences and begin healing;
- Reported increase in intrapersonal/informal community supports as knowledge of impacts spreads in communities (i.e. an increase in social support and social cohesion, an aspect of social capital);
- Reported improved family relationships as a result of control of negative emotions and heightened empathy resulting from increased knowledge of IRS effects;
- Reuniting of mothers and children taken into care after mothers completed healing programs;
- Less tolerance for sexual abuse at the community level, attributed to increased disclosures and heightened sense of personal pride and autonomy ("empowerment");
- Reported increase in connections between Elders and youth, particularly those intergenerationally impacted;
- Many respondents noted the program enabled them to live life more fully; the comment often made was "this program saved my life!"
- The beginning of hope for positive change; and
- In many cases, increased cooperation between social/health agencies indicated by cross-referrals, shared training, shared resources.
3.2.2 Impacts of the Settlement Agreement on Healing Needs
As the focus of this evaluation is on the funding arising from the Settlement Agreement, and the funding period from its inception until the present, the impacts of this significant change in the context of Aboriginal healing from IRS was identified as an evaluation issue to investigate. The challenges to program administration and delivery attributed to the effects of the Settlement Agreement processes are discussed above; here we outline the most frequent responses to the question: "Since the Settlement Agreement has been in place, and compensation of various kinds has been offered, do you think this has had effects on the healing needs of communities, and if so, what would those effects be?"
The majority of respondents felt that the Government's formal apology had had a significant impact at the personal, community and national level. For some Survivors, this was the recognition and acknowledgement of their suffering that they had been awaiting for a long time; some reported that the heightened awareness caused by the Apology made them feel at last entitled to come forward for healing; the government Apology in a sense gave public authenticity to the private pain and shame many Survivors had endured for most of their lives. Some respondents, however, reported that the Apology had "opened up old wounds" that had been closed as a means of psychological survival.
From the perspective of AHF headquarters and project directors, one of the most significant impacts of the Settlement Agreement processes is the increase in demand for help from Survivors who are in the IAP process or contemplating doing so, or have had effects from the CEP payment, or are looking for information. Interviewees from Survivors' societies also noted very high level of demand for help and information from Survivors experiencing confusion or negative effects from the compensation processes.
A number of respondents commented that financial compensation cannot heal trauma, or that "no amount of money can undo the harm that was done". Some Survivors commented that they would prefer to have an apology from those who did the harm.
Overall, both positive and negative impacts of the Settlement Agreement were noted; however, more negative than positive outcomes were reported for the compensation processes (CEP and IAP). To summarize, impacts identified by respondents (including case study interviewees) included the following:
Reported positive outcomes:
- Improvement in material circumstances for those able to cope with the sudden change in circumstances;
- Survivors feeling that their experience has been validated through public acknowledgement; and
- Seeking of healing for the first time for many who had repressed/denied their abuse.
Reported negative outcomes include:
- Increase in substance abuse and/or accidental death and suicide;
- Financial abuse of compensation recipients, particularly the elderly;
- Increase in negative feelings (anger, shame);
- "Outing" of Survivors to the community before they feel ready (i.e. by receiving a payment, status as Survivor becomes known);
- Those dealing with the effects for the first time (triggered by S.A. processes) exerting high pressure on the services of existing projects who have limited resources; and
- Victims of abuse report feeling re-victimized by the CEP and IAP process. Of particular note, a number of respondents reported being frustrated by having their attendance at IRS questioned; by lost files that delayed the process; or by having to re-tell the details of their abuse.
3.3 Relevance
The chief question that helps to determine the relevance of the program is whether the need for the program still exists. Accordingly, the evidence gathered to demonstrate relevance, documents community needs and, by implication, the demand for AHF healing programs in communities.
Background:
The AHF Final report identifies 36 months as the minimum time to move through needs identification, outreach and initiation of therapeutic healing (AHF Final Report 2006). AHF research/evaluations suggest that, to heal from residential school abuse, an Aboriginal community requires an average of ten years of ongoing healing support (AHF 2009-2014 Corporate Plan; Degagné 2008). The AHF Final Report (Volume II, 2006) reported addictions, history of abuse as a victim, poverty, denial and grief as the most severe participant challenges (reported by over 50 percent of projects).
The current high demand for help and support reported by the AHF and Survivor Societies indicates that the level of need for mental health supports for Survivors in the Settlement Agreement processes is high. Health Canada's IRS Resolution Health Support Program (RHSP) helps to meet this demand through the provision of mental health and emotional supports to former students and their families throughout all phases of the Settlement Agreement, including those eligible or currently resolving claims through the IAP, CEP recipients and those participating in the truth and reconciliation or commemorative initiatives. In anticipation of the Settlement Agreement's implementation, the IRS RHSP was enhanced in November 2006 ($94 million over six years). Notable changes include the expansion of the eligibility criteria to include approximately 80,000 former IRS students and the addition of cultural support providers. (Treasury Board of Canada 2006).
Of the 145 currently funded projects, 23 percent are sure they will not be able to continue once AHF funding ends, and 56 percent of projects are unsure of their future without AHF funding (AHF 2009-2014 Corporate Plan).
3.3.1 Is There a Continued Need For The Program?
Data from the sample of project files reviewed (n=29) indicate the number of "serious challenges" present in communities in which AHF funded projects are operating. The close links between these social determinants of health and an individual's ability to heal are identified in the literature. [Note 38] It is notable that "unresolved grief" (often spoken of together with "loss") is the second most frequently identified challenge in20 08/09 reports; this speaks to the level of psychological trauma that program reporters understand to be occurring in their communities.
Figure 23, below, illustrates the challenges identified by the sample of projects reviewed (n=29) for the period under review (2007-2009), showing that high levels of healing needs persist.Figure 23: Community Indicators – Identified Serious Challenges
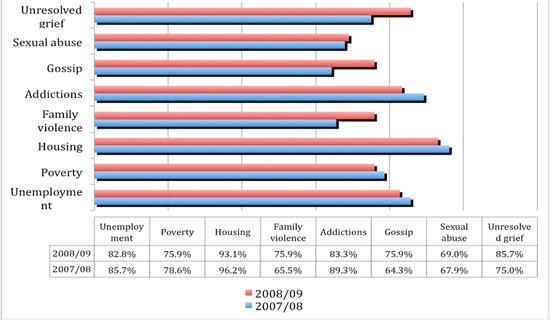
Figure 23: This figure shows a graph indicating the types of serious challenges facing AHF project communities. Data collected for the years 2007-08 is represented by one colour on the graph and data collected for the years 2008-09 is represented by another. In 2007-08, 85.7% of sample projects reviewed identified unemployment as a serious challenge present in their community; 78.6% identified poverty; 96.2% identified housing; 65.5% identified family violence; 89.3% identified addictions; 64.3% identified gossip; 67.9% identified sexual abuse and 75.0 % identified unresolved grief. In 2008-09, 82.8% of sample projects reviewed identified unemployment as a serious challenge present in their community; 75.9% identified poverty; 93.1% identified housing; 75.9% identified family violence; 83.3% identified addictions; 75.9% identified gossip; 69.0% identified sexual abuse and 85.7 % identified unresolved grief.
Interview Findings:
Several key respondent interviewees emphasized that, as the CEP / IAP and TRC processes will be ongoing for at least three more years, the AHF healing programs will be needed for at least that length of time.
Interviewees also noted frequently that the healing needs already addressed are "just the tip of the iceberg"; that the effects of IRS are far more widespread than first realized, including third and fourth generation family members. Inadequate parenting skills, addictions, and family violence are some of the most often cited social ills that interviewees attribute to IRS effects radiating down through families from IRS attendees who were traumatized. The disconnection from culture and language were also reported by many respondents as key factors in life trauma, and consequently, their restoration is seen to be a key to healing.
Another variable used as an indicator of continued need for IRS healing programs is the extent of community capacity and program alternatives to the AHF programs for addressing the healing needs of IRS Survivors and others impacted by IRS effects. Figure 24, below, illustrates the reporting of these indicators by the sample of projects reviewed (n=29). As the graph shows, reported levels of family violence are still high in the communities reporting, and rose substantially between the two reporting periods. This concurs with comments made by a number of interviewee respondents, who feel that abuse and family violence directly attributable to IRS effects, but in the children and grandchildren of Survivors, are still growing and represent the next big challenge for healing.
Figure 24: Community Indicator – Community Capacity Challenges
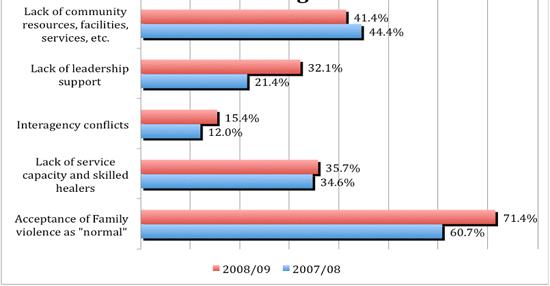
Figure 24: This figure shows a graph indicating the challenges to community capacity reported by sample AHF projects. Data collected for the years 2007-08 is represented by one colour on the graph and data collected for the years 2008-09 is represented by another. In 2007-08, 60.7% of project reported that acceptance of family violence as "normal" was a challenge to community capacity; 34.6% reported lack of service capacity and skilled healer; 12.0% reported interagency conflicts; 21.4% reported lack of leadership support and 44.4% reported lack of community resources, facilities, services, etc. In 2008-09, 71.4% of project reported that acceptance of family violence as "normal" was a challenge to community capacity; 35.7% reported lack of service capacity and skilled healer; 15.4% reported interagency conflicts; 32.1% reported lack of leadership support and 41.4% reported lack of community resources, facilities, services, etc.
Figure 25, below, indicates the data on the demand for healing services that was extracted from the sample of project files; this indication of high and growing demand for healing services is consistent with results of interviews at case study sites and comments made by other key respondents interviewed.
Figure 25: Community Indicator – Healing Demand

Figure 25: This figure shows a graph indicating data on the demand for healing services in sample AHF projects. Data collected for the years 2007-08 is represented by one colour on the graph and data collected for the years 2008-09 is represented by another. In 2007-08, two projects reported that there was no demand for healing services; thirteen projects reported an emerging demand and thirteen projects reported an established demand. In 2008-09, no projects reported that there was no demand for healing services; ten projects reported an emerging demand and twenty projects reported an established demand.
Many interviewees, as noted above, indicated that the healing "has just begun" and that only a fraction of the healing needs have been identified to date. The AHF has learned through its extensive research that the "healing journey" is long, complex and non-linear, and the healing needs of traumatized people require ongoing support and aftercare. Disclosure of physical and sexual abuse, which is noted as one of the first steps in the healing process, is ongoing in the community projects reviewed, as illustrated in Figure 26, below. In 2008/09, 59 percent of projects (n=17 of 28) reported that disclosure of physical and sexual abuse was established within their community; and such disclosure reportedly progressed from "emerging" to "established" in 17 percent of projects between 2007/08 to 2008/09.
Figure 26: Community Indicator – Disclosure of Physical and Sexual Abuse [Note 39]
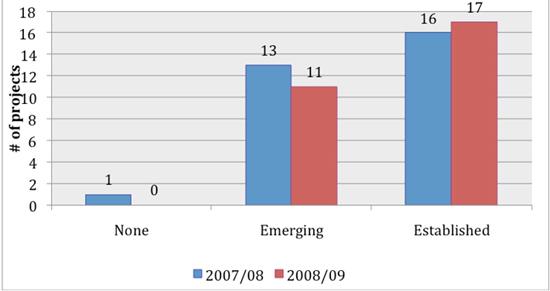
Figure 26: this figure shows a graph illustrating the disclosure of physical and sexual abuse in AHF project communities. Data collected for the years 2007-08 is represented by one colour on the graph and data collected for the years 2008-09 is represented by another. In 2007-08, one project reported that there was no disclosure of physical and sexual abuse; thirteen projects reported an emerging trend of disclosure and sixteen projects reported an established trend of disclosure. In 2008-09, eleven projects reported an emerging trend of disclosure of physical and sexual abuse and seventeen projects reported an established trend of disclosure. [Note 40]
In terms of overall demand, the majority of case study sites reported that demand exceeds their capacity to provide service (funds, staff, space); waiting lists were reported for some projects.
Data from the sample of project files reviewed indicates that program participation continues to grow overall; however, participation in healing circles, as one form of healing, appears to have dropped somewhat (see Figure 27, below). Comments provided on Annual Reports show that of the four projects whose healing circle participation rates dropped, one is a healing centre; one a community undergoing political stress; and one reported having to divert resources from healing to address CEP and IAP issues with Survivors. Interview findings indicate that healing circles would often be the first mode of healing accessed by participants; progress to other kinds of healing, or referrals to other kinds of help (e.g. individual counselling) would often be a subsequent step.
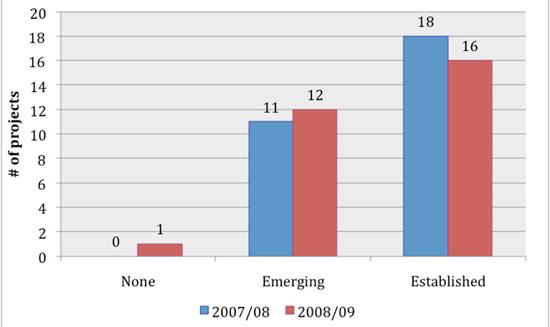
Figure 27: This figure shows a graph indicating program participation in healing circles in sample AHF project communities. Data collected for the years 2007-08 is represented by one colour on the graph and data collected for the years 2008-09 is represented by another. In 2007-08, eleven projects reported an emerging participation in healing circles and eighteen programs reported an established participation. In 2008-09, one project reported that there was no participation in healing circles; twelve reported an emerging participation and sixteen reported an established participation.
When asked if there is still a need for healing from the effects of IRS in their community, 99 percent of respondents replied that there is. When asked to estimate the percentage of people in their community they believe need healing from the effects of IRS, 89 percent of respondents answered "more than 50 percent".
In the opinion of most respondents, the healing "has just begun"; in particular, the needs of youth and others intergenerationally impacted are just beginning to be realized and addressed. A mental health expert consulted cited the Aboriginal suicide rate, one of the highest in the world, as evidence of the continued need for healing. The wider literature on Aboriginal suicide makes a direct link between sexual abuse and suicide in Aboriginal communities. [Note 41]
Rising enrolments (40 percent average increase over the 29 files reviewed) indicate a growing need for healing programs. Of 29 project files reviewed, only one reported no increase in participation. Case study interviews also confirmed rising enrolments.
Basing its projection on data from the Regional Health Survey, [Note 42] the AHF estimated (in 2006) the numbers of Aboriginal people needing healing to be 186,675 (AHF Final Report, Vol.I, 199).
3.3.2 Consequences of Closing The Program
When asked what the consequences would be if their program were to end, many respondents became visibly disturbed at hearing the question and contemplating the loss of the program. The vast majority of respondents in case studies used words such as "catastrophic", "disastrous" "a betrayal of trust"; "removal of hope" and other equally strong language to indicate their belief that ending the AHF healing programs at this point would have extremely negative consequences. Many respondents fear that individuals and communities will go back to previous states of being, as the healing is not yet widespread enough or firmly enough established. One program participant remarked that "people will wonder where to go now; there is nowhere else to go" (FNHH Case Study report). An Elder, in pointing out how long the history of trauma and abuse has been, said that "we had 100 years of abuse and 12 [sic] years of healing".
Experts and other key informants reiterated this view, pointing out that there are no current alternatives to the AHF in terms of community-based, culturally appropriate, effective healing directed at the effects of IRS. As noted above, one of the goals of the AHF has been to build the healing capacity in communities, but the majority view is that the goal is only partly achieved at this point and much more remains to be done.
4.0 Cost Effectiveness
An analysis of cost effectiveness considers whether the most appropriate and efficient means are being used to achieve objectives, relative to alternative design and delivery approaches. The evaluation cannot provide a valid cost-effectiveness analysis for the following reasons:
- Annual and quarterly project reports did not include sufficient detail to allow a meaningful analysis;
- The evaluation was under time constraints that did not allow time for analysis of further data; and
- In order to do a cost-effectiveness analysis, the cost of delivering the AHF programs would have to be compared to the cost of the same services provided by another program or department. There is no equivalent to AHF programs at the community or national level to make such a comparison.
That being said, there are some indications of the cost effectiveness of community-based healing programs that can be instructive, from a study of a successful community-based healing program at Hollow Water First Nation in Manitoba. A comparison of Aboriginal community-based healing of sexual abuse (Hollow Water Community Holistic Circle Healing) [Note 43] and equivalent government-run services shows that community-based healing cost anywhere from $4 to 13 million less to deliver over the ten year period. The study also points out that there are value-added benefits to Aboriginal-run community-based healing that would not normally be accounted for in a cost-effectiveness analysis, such as increases in social support and social cohesion and capacity; reduced crime, and other social benefits. As discussed in various sections of this report, such benefits have been identified in this evaluation as outcomes of AHF community-based programs. Furthermore, it is challenging to project the economic benefits of healing in terms of those who have become more productive by returning for further education or securing good employment as a result of undergoing healing; but this would likely reduce social service costs and have productive benefits. Certainly in the case study component of this evaluation we heard such reports from program participants, and this would be a useful avenue of research for the AHF to pursue, should it continue to be funded.
The AHF's research shows that by applying the Law Commission of Canada's economic model (2003) on the annual cost of child abuse to Canadian society (Calculated based on costs of incarceration, social services, special education and health), Survivors of residential school and those intergenerationally impacted could cost Canada $440 million per year (AHF Final Report 2006, Vol.I, 209). (The study did not factor in the productivity benefits discussed above). The conclusion reached by the AHF is that "healing the legacy of residential schools is an economically sound alternative" (2006, Vol.I, 209).
Another factor to consider in an assessment of community projects cost-effectiveness is the degree of in-kind support from community volunteers, enabling higher level of service delivery than funding amounts would warrant. Another factor noted by some interviewees is that, under the funding model, which closely resembles an endowment, the predictability and stability of project funds, versus year-by-year funding patterns of many government-funded programs, is able to save a great deal of human time and effort normally spent in completing funding applications on a yearly or more frequent basis.
Interview respondents note that the Foundation model used by the AHF has been cost-efficient by allowing for investment and using the interest to increase the effectiveness of funding (although the Funding Agreement conditions placed constraints on investment scope). Earned investment income is used for administration, which allowed 100 percent of the capital (plus some earned interest) to go to projects. The AHF notes that its administrative cost margin is below 15 percent.
5.0 Future Directions
Background:
Article 8.02 of the Settlement Agreement states that "Canada agrees that it will continue to provide existing mental health and emotional support services and agrees to make those services available to those who are resolving a claim through the IAP or who are eligible to receive compensation under the Independent Assessment Process. Canada agrees that it will also make those services available to Common Experience Payment recipients and those participating in truth and reconciliation or commemorative initiatives (Indian Residential Schools Settlement Agreement 2006).
Themajority of interviewees commented that, since the AHF has worked so well, why change it or discontinue its funding? The AHF has been noted as having achieved excellence in governance, [Note 44] and is cited internationally as an effective organization. One of the advantages cited by many respondents is the non-political nature of the AHF, which is structurally designed to remove some of the traditional barriers to cooperation than can occur. Another significant reported advantage to the AHF as the body to lead IRS healing initiatives is its Aboriginal and community-based nature, which is seen by Survivors and others as more accessible and trustworthy than government. In the opinion of most key informants (outside of the case studies) both inside and outside of government, there is a continued need for the healing work, research and knowledge dissemination that has been provided by the AHF, in the manner in which they have been doing so. That being said, in a renewed mandate there would be some new directions that could be taken by the AHF, according to key informants, as noted below.
5.1 Other Options, Alternatives, or Changes That Could Achieve Desired Outcomes
In a renewed mandate, some suggestions have been made as to new directions or approaches that might effectively benefit community-based projects.
Changes suggested by key informants include:
- Possible alternatives to the current funding arrangement would include adjusting the current funding parameters so that AHF could source alternative funds in the private and non-government organziation sector (including Aboriginal groups) in addition to government funding, while maintaining the high level of accountability AHF has historically shown.
- In support of the objective of capacity building, particularly with respect to increasing the mental health/healing human resource capacity nation-wide, the AHF could partner with agencies such as Health Canada, the Mental Health Commission of Canada and the Native Mental Health Association to support and implement the development of a culturally consonant mental health/healing human resources strategy.
- In a renewed mandate, it is suggested by some respondents that, because the needs are still high, and many Aboriginal communities were unable to access project funds, AHF should fund new projects. New projects could benefit from the sharing of promising practices mentioned above.
- Future research should make a systemic investigation of the community context and the social determinants of health in order to provide baseline information that can inform evaluations of healing program effectiveness. It will be difficult to estimate the community-level effects of AHF projects without accurate data on social indicators in communities. AHF could partner with another research organization (StasCan, NAHO or CIHI) in such an initiative.
6.0 Conclusions
A number of indicators provide evidence that AHF healing programs at the community level are effective in facilitating healing at the individual level, and are beginning to show healing at the family and community level; one of the variables in this is the length of time programs have been in operation; for example, most Inuit programs had a later start than others.
A substantial increase (average 40 percent) in program enrolments (from project file review) and stated by case study interviewees, indicate an increasing need for programs; this is supported by AHF research on projected community healing needs.
More youth are being engaged now than in the past; this is seen as an indicator of growing community capacity. Other indicators of the growth of community capacity reported by AHF projects are increased volunteerism and the growth of informal helping networks;
Impacts of the programs are reported as positive by the vast majority of respondents, with results ranging from increased self-esteem and pride; achievement of higher education and employment; to prevention of suicides.
It was noted by many that one of the most profound impacts of the healing programs (and the Apology) is that the "silence" and shame surrounding IRS abuses are being broken, creating the climate for healing; because this is just starting to happen in some communities, the healing trajectory will be longer than first anticipated.
The majority response is that the healing is gaining momentum, but that in relation to the existing and growing need, the healing "has just begun"; project reports and interview results indicate a high level of continued need for healing according to an array of negative social indicators attributed to IRS trauma.
The CEP, IAP and TRC are increasing the need for healing by "opening up" the issue for many Survivors for the first time, and as these processes will be ongoing for at least three years, the healing supports will be needed across the board; including a combination of professional mental health supports as well as community based healing programs.
Programs have been challenged over the long term by uncertainty regarding committed funding; shortages of trained/qualified staff; lack of resources for necessary follow-up care; and barriers to access such as childcare and transportation costs.
The majority of projects note they are not sustainable without AHF funding, although efforts are being made in some cases to secure funding from other sources.
Respondents note that there are few if any viable alternatives to achieve the positive healing outcomes the AHF has been able to achieve with such a degree of success.
Given the Settlement Agreement commitment by the GOC, and keeping in mind the assessments of the number of Survivors and intergenerationally impacted who are anticipated to need support; and the fact that Health Canada support programs are designed to provide specific services that are complementary but different to those of the AHF; and the reported numbers of Survivors seeking help from AHF and Survivor Societies, the logical course of action for the future would seem to be continuation of support for the AHF, at least until the Settlement Agreement compensation processes and commemorative initiatives are completed. Expert key interviewees note that there is no equivalent alternative that could achieve the desired outcomes with the rate of success the AHF has achieved.
7.0 Recommendations
It is recommended that:
- The Government of Canada should consider continued support for the Aboriginal Healing Foundation, at least until the Settlement Agreement compensation processes and commemorative initiatives are completed.
- The Government of Canada explore options with the Aboriginal Healing Foundation to determine how best to maximize any additional resources, should they become available, in order to be better able to meet the healing needs of Aboriginal Canadians.
- The Government of Canada undertake a study, in partnership with the Aboriginal Healing Foundation, research organizations, and stakeholders, to determine the healing needs of Aboriginal Canadians post Indian Residential Schools Settlement Agreement and determine whether funding should be continued and, if so, to what extent, and what role, if any, the Government of Canada should play.
- The Government of Canada implements, in the funding agreement with the Aboriginal Healing Foundation, a requirement to collect data to help determine cost effectiveness of community-based healing projects supported by the Foundation. They should also examine the possibility of a mandate to conduct strategic research and evaluation activities; however, this enhanced mandate should not detract from funding that would normally flow to community-based projects.
Literature & Documents Consulted
Literature Reviewed
Alianait Inuit-Specific Mental Wellness Task Group. 2007. Alianait Inuit Mental Wellness Action Plan.
Andersson, Neil and Robert J. Ledogar. 2008. The CIET Aboriginal Youth Resilience Studies: 14 Years of Capacity Building and Methods Development in Canada. Pimatisiwin: A Journal of Aboriginal and Indigenous Community Health, Vol. 6, # 2, 65-88.
Australian Human Rights Commission. 2008. Social Justice Report 2008, Chapter 4: Beyond the Apology- an agenda for Healing.
Bartlett, Judith G. 2003. "Involuntary Cultural Change, Stress Phenomenon and Aboriginal Health Status. Canadian Journal of Public Health Vol. 94, No.3.
Brown, Gregory P. 2003. Final Report. Evaluation of the Webequie First Nation Case Management Model. Prepared for the Intergovernmental Committee on Aboriginal Youth Suicide, March 31, 2003.
Campbell, Rebecca, Adrienne E. Adams and Debra Patterson. 2008. Methodological Challenges of Collecting Evaluation Data From Traumatized Clients/Consumers, A Comparison of Three Methods. American Journal of Evaluation, Vol.29, No. 3, September 2008, 369-381.
Castellano, Marlene Brant and Linda Archibald. 2006. Healing Historic Trauma: A Report from the Aboriginal Healing Foundation.
Castellano, M.; Archibald, L. & M. DeGagné. 2008. From Truth to Reconciliation: Transforming the Legacy of Residential Schools. AHF Research Series. Prepared for the Aboriginal Healing Foundation
Chasonneuve, Deborah. 2005. Reclaiming Connections: Understanding Residential School Trauma Among Aboriginal People. Prepared for the Aboriginal Healing Foundation
Chasonneuve, Deborah. 2007. Addictive Behaviours Among Aboriginal People in Canada. AHF Research Series. Prepared for the Aboriginal Healing Foundation.
Corrado, R. & I. M. Cohen. 2003. Mental Health Profiles for a Sample of British Columbia's Aboriginal Survivors of the Canadian Residential School System. AHF Research Series. Prepared for the Aboriginal Healing Foundation.
Couture, Joe; Parker,Ted; Couture,Ruth; and Patti Laboucane. 2001. A Cost-Benefit Analysis of Hollow Water's Community Holistic Circle Healing Process. Ottawa, Ontario: Ministry of the Solicitor General and the Aboriginal Healing Foundation.
Cox, Dorinda. No Date. Presentation on Aboriginal Healing Project: Rural and Remote Mental Health Conference, Gerldton. Department of Health WA
DeGagné, Michael. 2007. Toward an Aboriginal Paradigm of Healing: Addressing the Legacy of Residential Schools. Australasian Psychiatry, Vol. 15, pp. 49-53.
DeGagné, Mike. 2008. Administration in a National Aboriginal Organization: Impacts of Cultural Adaptations. Canadian Public Administration, Vol. 51, No. 4, pp. 659-672
Department of Justice Canada. 2008. Making the Criminal Justice System More Responsive to Victims Accessed online July 8, 2009.
Department of Justice Canada. 2009. Report on "Forum on Justice System Responses to Violence in Northern and Remote Aboriginal Communities" Accessed online July 8, 2009.
Dion Stout, Madeleine and Rick Harp. 2007. Lump Sum Compensation Payments Research Project: The Circle Rechecks Itself. Prepared for the Aboriginal Healing Foundation.
Environics Research Group. 2008. Final Report: 2008 National Benchmark Survey. Prepared for the Indian Residential Schools Resolution Canada and the Truth and Reconciliation Commission.
Fleming, John and Robert J. Ledogar. 2008. Resilience, an Evolving Concept: A Review of Literature Relevant to Aboriginal Research. Pimatisiwin: A Journal of Aboriginal and Indigenous Community Health, Vol.6, # 2, 7-23.
Fletcher, S. 2007. Communities Working for Health and Wellbeing: Success stories from the Aboriginal Community controlled health sector in Victoria. Victorian Aboriginal Community Controlled Health Organization and Cooperative Research Centre for Aboriginal Health.
Fletcher, F.; McKennit, D. & L. Baydala. No date. Community Capacity Building: An Aboriginal Exploratory Case Study. Pimatisiwin: A Journal of Aboriginal and Indigenous Community Health 5(2).
Government of Canada. May 8, 2006. Indian Residential Schools Settlement Agreement.
Government of Nova Scotia. 2002. Searching for Justice: An Independent Review of Nova Scotia's Response to Reports of Institutional Abuse Accessed online July 8, 2009.
Hawkeye Robertson, Lloyd. 2006. The Residential School Experience: Syndrome or Historic Trauma. Pimatisiwin: A Journal of Aboriginal and Indigenous Community Health 4(1) 2006
Health Canada. No date. Indian Residential Schools Resolution Health Support Program.
Indian and Northern Affairs Canada. 2008. Settlement Agreement Backgrounder.
Indian and Northern Affairs Canada. 2007. Update on the Settlement Agreement.
Indian and Northern Affairs Canada and the Aboriginal Healing Foundation. 2007. Funding Agreement.
Indian Residential Schools Adjudication Secretariat. 2008. Annual Report 2008.
Indian Residential Schools Settlement Official Court Website. Indian Residential Schools Class Action Litigation Accessed online July 8, 2009.
Indian Residential Schools Resolution Canada. 2008-2009. Report on Plans and Priorities.
Ing, Rosalyn N. 2000. Dealing with Shame and Unresolved Trauma: Residential School and its Impact on the 2nd and 3rd Generation Adults. A Doctoral Thesis, Dept. of Educational Studies, University of British Columbia
Inuit Tapiriit Kanatami. 2007. Inuit Statistical Profile.
Inuit Tapiriit Kanatami. 2008. 2007-2008 Annual Report.
Inuit Tapiriit Kanatami. 2009. 2008-2009 Annual Report.
Inuit Tapiriit Kanatami. 2009. Inuit Approaches to Suicide Prevention;
INAC. Integrated RMAF/ RBAF.Inuit Tapiriit Kanatami and Nunavut Research Institute. 2007. Negotiating Research Relationships with Inuit Communities: A Guide for Researchers.
Jiwa, A.; Kelly, L. & N St. Pierre-Hansen. 2008. Healing the community to heal the individual: Literature review of aboriginal community-based alcohol and substance abuse programs. Canadian Family Physician Vol. 54
Kelly, K. 2004 Surviving Traumatic Stress: A Guide for Multidisciplinary Remote and Rural Health Practitioners and their families
King, David. 2006. A Brief Report of the Federal Government of Canada's Residential School System for Inuit. Prepared for the Aboriginal Healing Foundation.
Kipling, G. & M. Dion Stout. 2003. Aboriginal People, Resilience and the Residential School Legacy. Prepared for The Aboriginal Healing Foundation.
Kirmayer, Laurence J., Gregory M. Brass, Tara Holton, Ken Paul, Cori Simpson. 2007. Suicide among Aboriginal People in Canada. Aboriginal Healing Foundation Research Series. Ottawa: The Aboriginal Healing Foundation.
Kishk Anaquot Health Research. 2001. Community Guide to evaluating Aboriginal Healing Foundation Activity. Prepared for Aboriginal Healing Foundation.
Kishk Anaquot Health Research. 2001. An Interim Evaluation Report of Aboriginal Healing Foundation Program Activity. Prepared for the Aboriginal Healing Foundation.
Kishk Anaquot Health Research. 2002. Journey and Balance: Second Interim Evaluation Report of Aboriginal Healing Foundation Program Activity. Prepared for the Aboriginal Healing Foundation.
Kishk Anaquot Health Research. 2003.Third Interim Evaluation Report of Aboriginal Healing Foundation Program Activity. Prepared for the Aboriginal Healing Foundation.
Korhonen, Marja. No Date. Culturally Sensitive Counselling With Inuit: An Example of Practical Application of Research. National Aboriginal Health Organization.
Kowanko, I. & C. Power. 2008. Central Northern Adelaide Health Service Family and Community Healing Program: Evaluation Report 31 March 2008. Flinders University, Adelaide.
Lane, Phil Jr., Michael Bopp, Judie Bopp, and Julian Norris. 2002. Mapping the Healing Journey: The Final Report of a First Nation Research Project on Healing in Canadian Aboriginal Communities APC 21 CA (2002) Aboriginal Corrections Policy Unit. Department of the Solicitor General. Ottawa: Supply and Services Canada.
Law Courts Education Society of BC. 2005. Understanding the Survivors Experience.
Law Courts Education Society of BC. 2005. Needs of the Survivors of Institutional Abuse.
Law Courts Education Society of BC. 2005. Healing Options for Survivors.
Law Courts Education Society of BC. 2005. Community Initiatives.
Law Courts Education Society of BC. 2005. Comparing Options.
MacDonald, Rob. 2006. First Nations Child and Family Caring Society of Canada Program Evaluation Research: Final Report. First Nations Child and Family Caring Society of Canada.
Manson, Spero, Janette Beals, Theresa O'Nell, Joan Piasecki, Donald Bechtold, Ellen Keane and Monica Jones. 2001. Chapter 10 in Marsella, Anthony J, Matthew J. Friedman, Ellen T. Gerrity and Raymond M Scurfield (eds), Ethnocultural Aspects of Post Traumatic Stress Disorder: Issues, Research and Clinical Applications. Washington, D.C: American Psychological Association.
May, P.A.; Serna, P.; Hurt, L. & L.M. DeBruyn. 2005. Outcome Evaluation of a Public Health Approach to Suicide Prevention in an American Indian Tribal Nation. American Journal of Public Health, Vol. 95, No. 7, 1238-1244.
Mayne, John. 2008. Addressing Cause and Effect in Simple and Complex Setting through Contribution Analysis. Found in Schwatz, R.; Forss, K. & M. Marra, Evaluating the Complex
McEwan, A., Tsey, K. & the Empowerment Research Team. 2008. The Role of Spirituality in Social and Emotional Wellbeing Initiatives: The Family Wellbeing Program at Yarrabah, Discussion Paper No. 7, Cooperative Research Centre for Aboriginal Health, Darwin.
Menzies, Peter. 2007. Understanding Aboriginal Intergeneration Trauma from a Social Work Perspective. The Canadian Journal of Native Studies, 2007; 27, 2
Milloy, John. 1999. "A National Crime": The Canadian Government and the Residential School System, 1879-1986. The University of Manitoba Press.
Mussell, B.; Cardiff, K. & J. White. 2004. The Mental Health and Well-Being of Aboriginal Children and Youth: Guidance for New Approaches and Services. Prepared for the British Columbia Ministry of Children and Family Development.
Mussell, Bill and Vicki Smye. 2001. Aboriginal Mental Health: ‘What Works Best'. A Discussion Paper. Mental Health Evaluation and Community Consultation Unit, UBC.
National Aboriginal Health Organization. 2006. Suicide Prevention: Inuit Traditional Practices That Encouraged Resilience and Coping. Ajunnginiq Centre.
National Aboriginal Health Organization. 2007. Resilience: Overcoming Challenges and Moving on Positively. Ajunnginiq Centre.
Naut'sa mawt Resources Group Inc. and Quadra Planning Consultants Ltd. 2004. White Stone Program Evaluation Final Report. Prepared for National Aboriginal Policing Services Branch, RCMP..No Author. 2003. Cost-Benefit Analysis of a Community Healing Process. Corrections Research, Solicitor General of Canada.
Pauktuutit Inuit Women's Association. 2004. Abuse Prevention Services in Inuit Communities: Analytical Report. The Nuluaq Project: National Inuit Strategy for Abuse Prevention.
Pauktuutit Inuit Women's Association. 2004. Analysis Report: Inuit Healing in Contemporary Inuit Society. Final. The Nuluaq Project: National Inuit Strategy for Abuse Prevention
Pawson, Ray. 2002. Evidence-based Policy: The Promise of ‘Realist Synthesis'. Evaluation 8(3), 340-358.
Public Safety Canada. 2008. An Evaluation of the Mamowichihitowin Community Wellness Program
Quinn, Ashley. 2007. Reflection on Intergenerational Trauma: Healing as a Critical Intervention. First Peoples Child & Family Review Vol.3, No. 4, 72-82.
Ralph, N.; Hamaguchi, K. & M. Cox. No Date. Transgenerational Trauma, Suicide and Abuse in Kimberley Region, Australia.
Robin, W. Robert, Barbara Chester and David Goldman. 2001. Cumulative Trauma and PTSD in American Indian Communities. Chapter 9 in Marsella, Anthony J, Matthew J. Friedman, Ellen T. Gerrity and Raymond M. Scurfield (eds). Ethnocultural Aspects of Post Traumatic Stress Disorder: Issues, Research and Clinical Applications. Washington, D.C: American Psychological Association.
Rogers, Patricia J. 2008. Using Programme Theory to Evaluate Complicated and Complex Aspects of Interventions. Evaluation 2008, 14 (1), 29-48.
Sampson, Alice. 2007. Developing Robust Approaches to Evaluating Social Programmes. Evaluation. Vol. 13(3), 477-493.
Shea, Goldie M. 1999. Redress Programs Relating to Institutional Child Abuse in Canada. Prepared for the Law Commission of Canada.
Tagalik, Shirley. 2006. Arviat: A Case Study of a Community Healing Process – An Analysis of the RespectED Abuse Prevention and Intervention Training Program. Mental Health Task Force: Government of Nunavut.
Tait, Caroline L. 2003. Fetal Alcohol Syndrome Among Aboriginal People in Canada: Review and Analysis of the Intergenerational Links to Residential Schools. AHF Research Series. Prepared for the Aboriginal Healing Foundation
Tatz, Colin. 1999. Aboriginal Suicide is Different. Aboriginal Youth Suicide in New South Wales, the Australian Capital Territory and New Zealand: Towards a Model of Explanation and Alleviation. A Report to the Criminology Research Council on CRC Project 25/96-7.
The Aboriginal Healing Foundation. 1998. Letters Patent.
The Aboriginal Healing Foundation. 2000. Ethics Guidelines for Aboriginal Communities Doing Healing Work
The Aboriginal Healing Foundation. 2001. Code of Conduct for Directors, Staff and Others Involved in the Work of the Foundation.
The Aboriginal Healing Foundation. 2001. Conflict of Interest Policy for Directors of the Aboriginal Healing Foundation.
The Aboriginal Healing Foundation. 2005. Annual Report 2005: Aboriginal Healing Foundation.
The Aboriginal Healing Foundation. 2006. The Aboriginal Healing Foundation 2006 Annual Report.
The Aboriginal Healing Foundation. 2006. Final Report of the Aboriginal Healing Foundation: Volume I, Marlene Brant Castellano: A Healing Journey, Reclaiming Wellness; Volume II, Kishk Anaquot Health Research: Measuring Progress, Program Evaluation; and Volume III, Linda Archibald: Promising Healing Practices in Aboriginal Communities. Ottawa, ON: Aboriginal Healing Foundation.
The Aboriginal Healing Foundation. 2007. 2007 Annual Report: Helping Aboriginal People Heal Themselves.
The Aboriginal Healing Foundation. 2007. Directory of Residential Schools in Canada.
The Aboriginal Healing Foundation. 2008. The 2008 Annual Report of the Aboriginal Healing Foundation.
The Aboriginal Healing Foundation. 2008. Active Funding Grants.
The Aboriginal Healing Foundation. Overview of the Aboriginal Healing Foundation's Final Report.
The Aboriginal Healing Foundation. No Date. The Aboriginal Healing Foundation 2009-2014 Corporate Plan.
The Aboriginal Healing Foundation. No Date. By-law Number 1, relating generally to the transaction of the affairs of the Aboriginal Healing Foundation.
The Nuluaq Project: National Inuit Strategy for Abuse Prevention.
Thomas, W. & G. Bellefeuille. 2006. An evidence-based formative evaluation of a cross cultural Aboriginal mental health program in Canada. Australian e-Journal for the Advancement of Mental Health, Vol. 5 Issue 3, 2006 ISSN: 1446-7984.
Treasury Board of Canada Secretariat. 2007. Evaluation of Foundations Accessed online July 8, 2009.
Treasury Board of Canada. October 19, 2006. Decision of the Treasury Board Meeting of October 19, 2006. Subject: Implementation of the Indian Residential Schools Settlement Agreement. (CONFIDENTIAL DOCUMENT provided by INAC to contractor)
Tungasuvvingat Inuit. 2007. Mamisarniq Conference 2007– Inuit-specific Approaches to Healing from Addiction and Trauma. Prepared for Inuit Tapiriit Kanatami.
Waldram, James B. 2008. Aboriginal Healing in Canada: Studies in Therapeutic Meaning and Practice. AHF Research Series. Prepared for National Network for Aboriginal Mental Health Research in partnership with the Aboriginal Healing Foundation
Waldram, James B. 2008. "The Models and Metaphors of Healing" in Aboriginal Healing in Canada: Studies in Therapeutic Meaning and Practice. The Aboriginal Healing Foundation Research Series. Ottawa: The Aboriginal Healing Foundation.
Wesley-Esquimaux, C. & M. Smolewski. 2004. Historic Trauma and Aboriginal Healing. AHF Research Series. Prepared for the Aboriginal Healing Foundation
Zamparo, J. & D.I.M. Spraggon. No Date. Echoes and Reflections: A Discussion of Best Practices in Inuit Mental Health – A Comparative Cross-Jurisdictional Analysis of the Literature on Services, Program Models, and Best Practices in Mental Health, With a Focus on Interdisciplinary, Intersectoral Approaches Emphasizing Inuit Youth. Government of Nunavut Task Force on Mental Health
Appendix A
Glossary of Terms [Note 45]
Aboriginal Healing Foundation (AHF)
The non-profit corporation established under Part II of the Canada Corporations Act chapter C-32 of the Revised Statues of Canada, 1970 to address the healing needs of Aboriginal People affected by the Legacy of Indian Residential Schools, including intergenerational effects.
Aboriginal People
Individuals who are included as Aboriginal peoples referred to in S. 35 of the Constitution Act1982 and, for greater certainty, include Inuit, Métis and First Nations, on and off reserve, regardless of whether they are registered under the Indian Act.
Board
The board of directors of the Foundation as constituted from time to time.
Capacity
The collective ability of residents in a community to respond to external and internal stresses, to create and take advantage of opportunities and to meet the needs of residents.
Capacity Building
Capacity building is an ongoing process through which individuals, groups, organizations and societies acquire the resources necessary to realize their socio-economic and political aspirations, work towards improving their psychological and/or emotional well-being and to effectively manage change to meet existing and future responsibilities.
Case Studies
Case studies emphasize detailed contextual analysis of a limited number of events or conditions and their relationships. A key strength of the case study method involves using multiple sources and techniques in the data gathering process. The information collected is primarily qualitative in nature, but it may also be quantitative. Tools to collect data include: interviews, focus groups, document review, surveys and observation. Case study research helps to increase our understanding of a complex issue and can add strength to what is already known through previous research.
Collaboration
The process by which people or organizations work together (i.e., engagement) to accomplish a common mission. Collaboration is the basis for bringing together the knowledge, experience and skills of a number of people or groups to contribute to a specific goal (e.g., strategy) more effectively than individuals/groups working in isolation.
Common Experience Payment (CEP)
A lump sum payment made to an Eligible CEP Recipient in the manner set out in Article Five of the Indian Residential Schools Settlement Agreement.
Community-based
Responding to the healing needs of Aboriginal communities, including Communities of Interest.
Communities of Interest
A body, collective, association, incorporation, coming together, or other amalgamation of Aboriginal People.
Elder
Someone who has special gifts. Elders are generally considered exceptionally wise in the ways of their culture. They are recognized for their wisdom, their stability, and their ability to know what is appropriate in a particular situation. The community looks to them for guidance and sound judgment. They are caring and are known to share the fruits of their labours and experience with others in the community. (RCAP Final Report, Vol. 4, Ch. 3 as citied in Aboriginal Healing Foundation Code of Conduct for Directors, Staff and Others involved in the work of the Foundation).
Eligible Costs
Means the costs of operating, managing and administering an Eligible Project subject to the provisions of Sec. 7.05 and 7.06 of the Funding Agreement for the Aboriginal Healing Foundation.
Eligible Project
Means a project carried on or to be carried on to address the healing needs of Aboriginal People affected by the Legacy of Indian Residential Schools, including the intergenerational impacts.
Eligible Recipient
Means an organization located in Canada or individual residing in Canada that carries on, or in the opinion of the Board is capable of carrying on, projects to address the healing needs of Aboriginal People affected by the Legacy of Indian Residential Schools, including the intergenerational impacts.
Endowment
Endowments are a funding instrument in which funds are provided in a lump sum for an extended time period, and the terms normally prohibit spending of the capital. The recipient of the endowment is allowed to use the interest earned on investment of the capital. The funding provided to AHF in 2007 is not, in strict terms, an endowment, although it is referenced in the Settlement Agreement as such.
Evidence-based Decision Making
Evidence-based decision making is the systematic application of the best available evidence to the evaluation of options and to inform decision making.
Foundation
Means the non-profit Aboriginal Healing Foundation established under the Canada Corporation Act to address the healing needs of Aboriginal People affected by the Legacy of Indian Residential Schools, including the intergenerational impacts. Foundations are defined (in Budget 2005) as "not-for-profit organizations governed by independent arms' length boards of directors made up of experienced and knowledgeable individuals with expertise in specific areas of research, development and learning. Their arm's length nature, financial stability and focused expertise allow them to address specific challenges in a highly effective non-partisan manner" [Note 46]
Funding Agreement
Means the Funding Agreement of the Aboriginal Healing Foundation providing for the ongoing relationships between the Parties to the Agreement and includes all schedules and exhibits.
Healing
According to the AHF, "Healing" can mean different things to different people. Healing occurs when an individual has meaningfully resolved the effects of trauma and has overcome patterns of destructive and self-destructive behaviour. The goal of healing is balance at all levels within persons and within their relationships. Healed individuals, families, and communities are able to create and sustain the conditions which promote their well being.
Historic trauma
A cumulative emotional and psychological wounding across generations resulting from significant and long-term tragedies [Note 47]
Indian Residential Schools "Indian Residential Schools"means the following:
- Institutions listed on List "A" to OIRSRC's Dispute Resolution Process attached as Schedule "E" of the Indian Residential Schools Settlement Agreement;
- Institutions listed in Schedule "F" ("Additional Residential Schools") which may be expanded from time to time in accordance with Article 12.02 of the Indian Residential Schools Settlement Agreement; and,
- Any institution which is determined to meet the criteria set out in Section 12.02(2) and (3) of the Indian Residential Schools Settlement Agreement. [Note 48]
Intergenerational Impacts
The effects of sexual, physical, mental and emotional abuse that were passed on to the children, grandchildren and great-grandchildren of Aboriginal people who attended the residential school system.
Key Interviews
Key interviews are those done with key individuals knowledgeable about the subject matter of a research study. Such interviews allow for the collection of knowledge, perceptions and opinions about a variety of evaluation issues including rationale, implementation and delivery, success, cost-effectiveness, and future considerations.
Legacy of the Indian Residential Schools ("Legacy")
Any continuing direct or indirect effects of Indian Residential Schools, including the intergenerational impacts, on individuals, families and communities, including Communities of Interest. These effects may include, and are not limited to, family violence, drug, alcohol and substance abuse, physical and sexual abuse, loss of parenting skills and self-destructive behaviours.
Post traumatic stress disorder (PTSD)
A diagnostic category used to describe a psychological disorder that develops in some individuals who had major traumatic experiences, such as those who experienced serious accidents, survived or witnessed violent crimes or acts of wars. Symptoms can include emotional numbness at first, depression, excessive irritability, guilt for having survived others who were injured or died, recurrent nightmares, flashback to the traumatic scene, and overreactions to sudden noises [Note 49] It is believed by some that Aboriginal PTSD is of a different order and should be given its own designation [Note 50]
Settlement Agreement
The final Indian Residential Schools Settlement Agreement reached by consensus between representatives of Canada, Plaintiffs, Independent Counsel, The Assembly of First Nations, Inuit Representatives, The General Synod of the Anglican Church of Canada, They Presbyterian Church of Canada, The United Church of Canada and Roman Catholic Entities.
Survivors
Individuals who attended and survived "Residential School" (as that term is defined by the Aboriginal Healing Foundation in its by-laws), their families or descendants or both. [Note 51]
Tri-Council Policy Statement
The Tri-Council Policy Statement: Ethical Conduct for research Involving Humans, describes standards and procedures for governing research involving human subjects. Section 6.0 – Research Involving Aboriginal Peoples – focuses specifically on the development of ethical standards and practices for carrying out research involving Aboriginal peoples, communities or groups.
Footnotes
- (The 2008 Annual Report of the Aboriginal Healing Foundation, p. 14) (return to source paragraph)
- AHF. 2006. Summary Points of the AHF Final Report. p. 8. (return to source paragraph)
- Indian Affairs and Northern Development Canada. 2000. "Gathering Strength – Canada's Aboriginal Action Plan". (return to source paragraph)
- Funding Agreement Aboriginal Healing Foundation and Her Majesty the Queen in Right of Canada, as Represented by the Minister of Indian Affairs and Northern Development and Federal Interlocutor for Métis and Non-Status Indians. Internal document provided to DPRA by INAC. (return to source paragraph)
- $25 million of this was in the form of a Contribution Agreement between the parties dated May 28, 2007; the additional $100 million was provided as a payment attached to a Funding Agreement between the GOC and the AHF. While this is referred to as a endowment in the Settlement Agreement, the Funding Agreement does not include this term, nor does it include the standard restriction on endowments that capital may not be disbursed, only invested. Under the terms of the Funding Agreement, capital was disbursed on a schedule to projects, and the remaining non-disbursed capital was invested. (return to source paragraph)
- Ibid. p5 (return to source paragraph)
- Institute on Governance. John Graham and Laura Mitchell. 2009. A Legacy of Excellence: Best Practices Board Study, Aboriginal Healing Foundation. Ottawa: Institute on Governance. (return to source paragraph)
- Ibid. p 4 (return to source paragraph)
- The Aboriginal Healing Foundation. 2006. A Healing Journey: Final Report.(return to source paragraph)
- Ibid. (return to source paragraph)
- Kishk Anaquot Health Research. 2001. An Interim Evaluation Report of Aboriginal Healing Foundation Program Activity. Prepared for the Aboriginal Healing Foundation. return to source paragraph)
- AHF Final Report Vol. I. (return to source paragraph)
- The Aboriginal Healing Foundation. 2005. Annual Report 2005. (return to source paragraph)
- The Aboriginal Healing Foundation 2008. The 2008 Annual Report of the Aboriginal Healing Foundation. (return to source paragraph)
- Clause 11.14 of the Funding Agreement between the AHF and the GOC also outlines the Minister's right to conduct a program evaluation. An evaluation under that particular clause would be a separate evaluation from this, if it were to be done. (return to source paragraph)
- This was not possible at First Nations House of Healing, Tsa Kwa Luten Lodge, as the evaluation took place during the summer, when the lodge is used as a tourist facility. The case study took place at the offices of Intertribal Health Authority in Nanaimo, B.C. (return to source paragraph)
- Michael Degagné notes this development of healing approaches "grounded in Indigenous knowledge" in a recent publication: Degagné, Michael. 2007. Toward an Aboriginal Paradigm of Healing: Addressing the Legacy of Residential Schools. Australian Psychiatry, Vol.15, Supplement. (return to source paragraph)
- See, for example: Castellano, Marlene Brant and Linda Archibald. 2006. Healing Historic Trauma. A Report from the Aboriginal Healing Foundation. In White, J.P; Maxim, P. & D. Beavon (Eds.), Aboriginal Policy Research: Volume IV Moving Forward, Making a Difference. Thompson Educational Publishing and also Ralph, Naomi et al. 2006. Transgenerational Trauma, Suicide and Healing from Sexual Abuse in the Kimberley Region, Australia. Pimatisiwin: A Journal of Aboriginal and Indigenous Community Health, Vol.4, # 2, 118-136. (return to source paragraph)
- The AHF research discovered early that healing is "of a greater intensity and duration than originally anticipated" (Kishk Anaquot Health Research. 2001. An Interim Evaluation Report of Aboriginal Healing Foundation Program Activity. Prepared for the Aboriginal Healing Foundation (return to source paragraph)
- "Emerging" is defined by the AHF for project reporters as: "Progress is just beginning and there are early indications of positive change". "Established" is defined as: "The situation or service described exists in the community and is working well." (AHF Project Annual Report Template) (return to source paragraph)
- Such cases are indicated in the report where applicable. (return to source paragraph)
- While reporters are directed to base their comments on the majority of communities, there is still room for ambiguity. AHF may want to address this reporting issue in a continued mandate. (return to source paragraph)
- Mayne, John. 1999. Addressing Attribution through Contribution Analysis: Using Performance Measures Sensibly. Office of the Auditor General Canada, June 1999. (return to source paragraph)
- The Aboriginal Healing Foundation. 2006. Final Report of the Aboriginal Healing Foundation, Volume I, A Healing Journey: Reclaiming Wellness. Ottawa: Aboriginal Healing Foundation. (return to source paragraph)
- The Aboriginal Healing Foundation. 2006. Final Report of the Aboriginal Healing foundation, Volume II, Measuring Progress: Program Evaluation, p.78. (return to source paragraph)
- Data not provided for Yellowknives Dene project for either year. Data not provided for Kuujuaq project for 07/08. (return to source paragraph)
- This data was not available for the Nunavik case study site for 07/08. (return to source paragraph)
- N=29, however one project removed from total due to reporting indicator as N/A; one project reported this indicator as both Emerging and Established. (return to source paragraph)
- N=28 due to one project being removed from total due to reporting indicator as N/A. (return to source paragraph)
- N=30 due to two projects reporting this indicator as both Emerging and Established; comments indicate that community engagement depends on level of sobriety and other individual factors. (return to source paragraph)
- N=30 because of one project reporting this indicator as both "None" and "Established"; comments indicate that this is because some leadership does participate and some does not. (This was also noted by other projects.) (return to source paragraph)
- N=31 due to one project reporting this indicator as both Emerging and Established, and another reporting both None and Emerging. Comments indicated that for some disclosure may be established, for others it is just beginning; and generally projects indicated that this indicator is different dependent on the individual and/or community. (return to source paragraph)
- N=30 due to one project reporting this indicator as both Emerging and Established. Comments indicated that for some disclosure may be established, for others it is just beginning. (return to source paragraph)
- Inuit Tapiriit Kanatami. 2007. Mamisarniq Conference 2007 – Inuit-specific Approaches to Healing from Addiction and Trauma, p.12. (return to source paragraph)
- The term "respondent" and "interviewee" are used interchangeably. (return to source paragraph)
- This finding is corroborated by findings of an evaluation of foundations (one of which was the AHF). See Treasury Board of Canada Secretariat 2007. Evaluation of Foundations. (return to source paragraph)
- N=27 due to one project reporting indicator as N/A, and one project leaving indicator blank on report; comments indicated in the second case that referrals did occur. (return to source paragraph)
- See: Tatz, Colin. 1999. Aboriginal Suicide is Different. Aboriginal Youth Suicide in New South Wales, the Australian Capital Territory and New Zealand: Towards a Model of Explanation and Alleviation. A Report to the Criminology Research Council on CRC Project 25/96-7. Accessed at: ; Ralph, N.; Hamaguchi, K. & M. Cox. 2006. Transgenerational Trauma, Suicide and Abuse in Kimberley Region, Australia; and May, P.A.; Serna, P.; Hurt, L. & L.M. DeBruyn. 2005. Outcome Evaluation of a Public Health Approach to Suicide Prevention in an American Indian Tribal Nation. American Journal of Public Health, Vol. 95, No. 7, 1238-1244. (return to source paragraph)
- Note: N=30 projects in 2007/08 because one project reported indicator as both Emerging and Established. The reason for this was reported to be that physical abuse was Established while sexual abuse was still Emerging. N=28 projects in year 2008/09 due to one project leaving indicator blank on Annual Report. Comments indicated that as people seek healing, others also seek help. (return to source paragraph)
- Note: N=28 projects in year 2007/08 due to one project leaving indicator blank on Annual Report.. N=30 projects in year 2008/09 due to one project reporting this indicator as both Emerging and Established; this project services several communities and comments indicated that status of demand for healing services depended on the particular community. (return to source paragraph)
- Tatz 1999 and Ralph et al 2006. (see footnote at p.31) (return to source paragraph)
- Source cited in AHF final report as: First Nations Regional Longitudinal Health Survey 2002-03. First Nations Information Governance Committee/Assembly of First Nations, First Nations Centre at the National Aboriginal Health Organization. (return to source paragraph)
- Couture, Joe, Ted Parker, Ruth Couture and Patti Laboucane. 2001. A Cost-Benefit Analysis of Hollow Water's Community Holistic Circle Healing Process. Ottawa, Ontario: Ministry of the Solicitor General and the Aboriginal Healing Foundation. (return to source paragraph)
- IOG 2009. (return to source paragraph)
- The list of terms defined in this section has been developed by the consultants and has been reviewed by the Advisory Committee. (return to source paragraph)
- Cited in Treasury Board of Canada Secretariat. 2007. Evaluation of Foundations. (return to source paragraph)
- Adapted from Linda Archibald 2006. Decolonization and Healing: Indigenous Experiences in the United States, New Zealand, Australia and Greenland. The Aboriginal Healing Foundation Research Series. (return to source paragraph)
- From Indian Residential Schools Settlement Agreement. May 2006. (return to source paragraph)
- From Linda Archibald, 2006. Decolonization and Healing: Indigenous Experiences in the United States, New Zealand, Australia and Greenland. Aboriginal Healing Foundation Research Series. (return to source paragraph)
- Robin, W. Robert, Barbara Chester and David Goldman. 2001. Cumulative Trauma and PTSD in American Indian Communities. Chapter 9 in Marsella, Anthony J, Matthew J. Friedman, Ellen T. Gerrity and Raymond M Scurfield (eds), Ethnocultural Aspects of Post Traumatic Stress Disorder: Issues, Research and Clinical Applications. Washington, D.C: American Psychological Association. (return to source paragraph)
- Ibid, p. 1 (return to source paragraph)
"Page details"
- Date modified: